
Table of Contents
The psychiatrist, seeing 25 patients a week, has a full booking. Claims are sent. Checks are in the mail. The clinic seems to be doing great, at least on the surface.
Because as soon as someone looks closely, he sees it.
The 99214 that SHOULD have been a 99215 based on how many criteria the document was met on the visit. The 90836 to bill added on to a 90837 visit, and it never was captured. The prior authorization expired 3 weeks prior, which means that all the visits I billed for since then, for 15 visits, will be denied post fact. The MBHO application was never submitted, and the 6 months of bills to that entity that should have been to the correct payer were sent incorrectly.
None of this presents itself to anyone.
It gathers, and GATHERS, until the damage is done. There is no “sound” of revenue leakage for a psychiatrist. Revenue leakage for a psychiatry group practice is quite silent and, if addressed, becomes mostly preventable for each practice.
Groups are doing it better, not necessarily by taking care of more clients/patients, but by taking care of their patients’ billing more carefully, more wisely about billing.
How Does Revenue Leakage Happen in Psychiatry Practices?
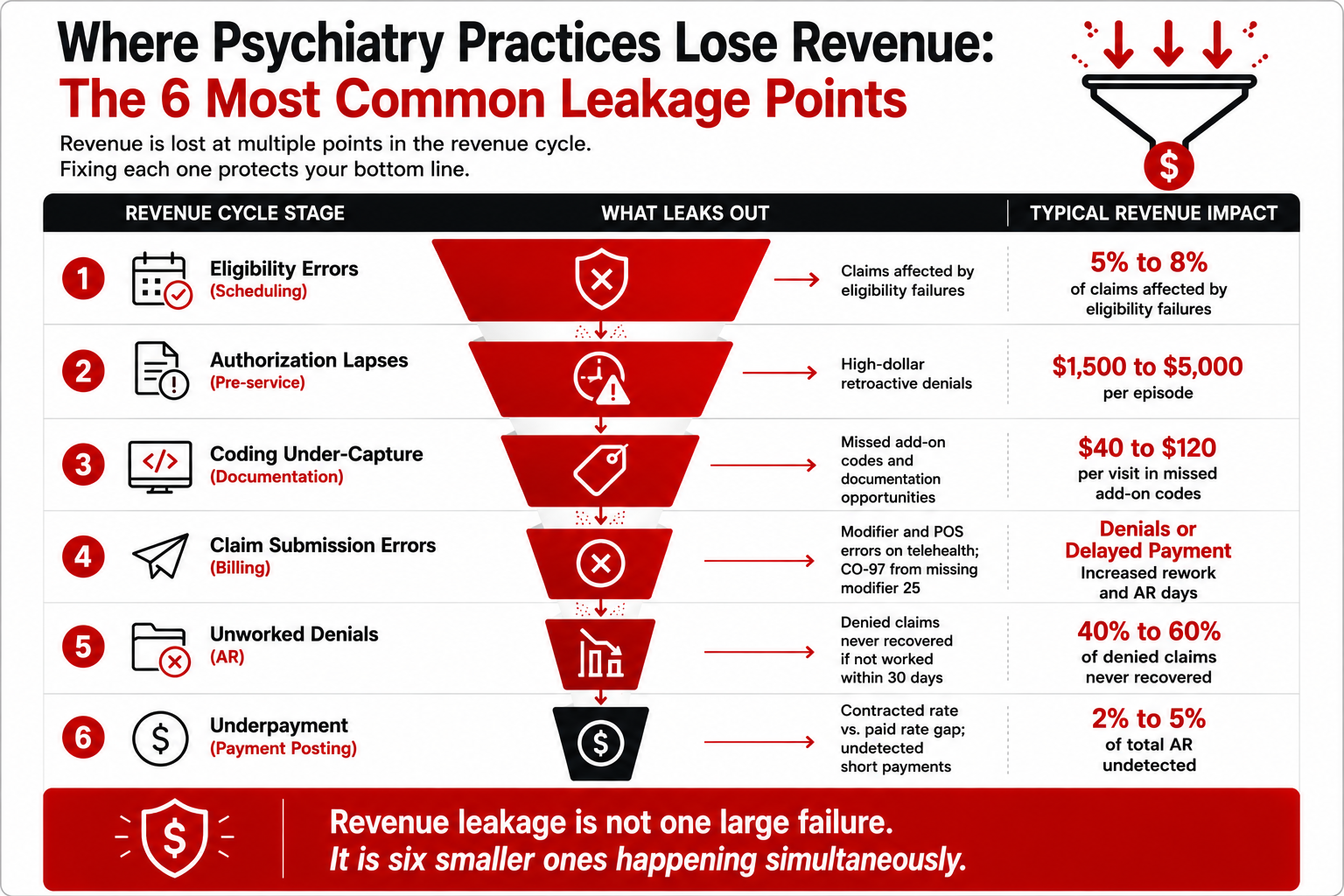
Revenue leakage in psychiatry is not one large failure. It is a collection of smaller, repeating ones:
- Under-coding E/M visits: Billing 99213 when 99214 is clearly supported by the clinical documentation; a conservative habit that costs $20 to $40 per visit
- Missing psychotherapy add-on codes: Not billing 90833, 90836, or 90838 on combined med management and therapy visits one of the most consistently underbilled opportunities in psychiatry
- Missing modifier 25: Billing 99214 + 90836 without modifier 25 on the E/M the claim bundles and the E/M is denied with CO-97
- Authorization lapses: Ongoing services (especially for complex patients requiring concurrent auth) billed after the authorization expires; retroactive denial across multiple sessions
- MBHO routing errors: Claims submitted to the base commercial payer when behavioral health is carved out to Optum BH, Carelon, or Evernorth; systematic denial across all affected patients
- Telepsychiatry billing errors: Wrong modifier (GT when payer requires 95) or wrong POS code (11 instead of 10), either denial or wrong reimbursement rate
- Unworked AR: Denied claims sitting in the queue past 60 days, approaching or past timely filing limits
Your Psychiatry Practice Is Probably Leaving $30K to $60K on the Table.
Under-coded E/M visits, missed add-on codes, MBHO enrollment gaps, and unworked AR are standard revenue leaks in psychiatry. BehavioralProz identifies them and closes them.
Which Billing Metrics Have the Biggest Impact on Psychiatry Revenue?
| KPI | Industry Benchmark | Revenue Impact | Why It Matters |
|---|---|---|---|
| Clean Claim Rate | 95% or higher | Every 1% below benchmark = 1% of billed charges requiring rework | First-pass acceptance determines billing efficiency |
| First-Pass Resolution Rate | 90% or higher | Below 85% signals submission or coding quality issues | Higher FPRR = faster payment and lower cost per claim |
| Days in AR | Under 35 days | Every additional 15 days in AR delays 15 days of cash flow per claim | Measures speed of the entire billing cycle |
| Net Collection Rate | 95% or higher | 1% below benchmark = $6,000/year lost per $600K in billings | Measures what is actually collected vs. what is owed |
| Denial Rate | Under 5% | Above 8% = systemic billing problem; every 3% above benchmark is significant AR exposure | Directly measures how many claims require second-cycle work |
| Authorization Approval Rate | 85% or higher | Below 75% suggests documentation or payer relationship issues | Auth denials create retroactive revenue exposure |
| Provider Utilization | Track against practice target | Providers seeing 20% fewer patients than target = proportional revenue reduction | Billing cannot recover revenue that was never generated |
Why Do Psychiatry Claim Denials Cost More Than Most Practices Realize?
The Cost of a denial is obvious, but the true cost of a denial can be many times that.
This is an example of how denials affect revenue for a psychiatry group practice:
- Monthly claim volume: 600 claims
- Average claim value: $175
- Denial rate: 10% (60 denied claims per month)
- Claims successfully appealed and recovered: 50%
- Monthly revenue permanently lost: $5,250
- Annual permanently lost revenue: $63,000
Not included in this figure is the administrative costs associated with researching and working the 60 denied claims per month; typical biller time is 2-4 hours a week, or about $8,000 to $15,000 in annual labor costs.
Total annual denial costs at a 10% denial rate: $71,000 to $78,000 for a practice with an annual billing of $1.26M.
Drop the denial rate to 5%, and the annual costs are approximately $35,000 to $39,000, a difference of about $36,000 due to process improvement alone!
How Does Under-Coding Reduce Psychiatry Revenue?
The stealthiest revenue loss in psychiatry. Under-coding doesn’t get a denial. It gets paid-just not paid what it could have been, based on the record.
Here are common psychiatry under-coding scenarios:
- 99213 billed for moderate complexity encounters that clearly support 99214 (30 to 39 minutes documented, or moderate MDM with medication changes)
- 99837 billed standalone for a combined visit when 99214 + 90836 was the correct code combination
- Add-on codes never billed because the biller did not realize the visit qualified
- 90792 billed for follow-up encounters instead of 99214 + add-on (a coding error in both directions)
Revenue example:
A psychiatrist billing 99213 for 15 visits per week that should be 99214:
- Average reimbursement difference: $28 per visit
- Weekly revenue loss: $420
- Annual revenue loss: $21,840
That is from one coding tier, for one provider. For a 5-provider group with the same pattern across the team, the annual under-coding loss reaches $109,200.
Why Does Credentialing Affect Psychiatry Collections?
Credentialing determines whether claims are paid at all. The most common credentialing-related revenue failures in psychiatry:
- MBHO not enrolled: Provider credentialed with Aetna but not Evernorth (Cigna’s MBHO). Claims denied with CO-B7 across all Evernorth patients until MBHO enrollment is completed.
- Enrollment not initiated at hire: Provider joins the practice, starts seeing patients, and the credentialing application is submitted on the start date. Payer approval takes 60 to 90 days. Every session during those 90 days is either unbillable in-network or billed at an out-of-network rate.
- CAQH profile expired: Re-attestation required every 120 days. Missed deadline silently suspends enrollment at every CAQH-connected payer simultaneously.
- PMHNP collaborative agreement: Some payers require a collaborative agreement with a supervising MD on file. Missing this suspends enrollment in states where it is a payer requirement, even if it is not a legal requirement.
RELATED READING


How Does Telepsychiatry Billing Influence Revenue Performance?
Telepsychiatry billing has more failure points per claim than in-person psychiatric billing. The most common:
Modifier errors:
- GT required by Medicare; 95 required by most commercial payers; submitting the wrong one generates a denial
- No modifier submitted at all: claim either denies or reimburses at wrong rate
POS code errors:
- POS 11 (office) billed for telehealth sessions triggers incorrect reimbursement or audit
- POS 10 (patient at home) required for most consumer telepsychiatry
Audio-only coverage:
- Medicare requires modifier FQ for audio-only behavioral health; many commercial plans require documentation of why video was unavailable
- Billing audio-only without confirming payer coverage generates a CO-4 denial
Revenue impact: A telepsychiatry practice billing 300 sessions per month with consistent POS errors is receiving either the wrong reimbursement rate or generating systematic preventable denials. At $175 average reimbursement, a 10% error rate is $5,250 per month in at-risk revenue.
What Revenue Opportunities Are Most Psychiatry Practices Missing?
Why Are Missed Authorizations Creating Revenue Loss?
Problem: Authorization obtained at admission; concurrent review deadline passed unnoticed. Sessions billed after expiration are denied retroactively.
Financial impact: A 10-session block denied post-auth-lapse at $175 per session is $1,750 per patient. For a practice with 5 patients in complex auth-required treatment at any given time, one lapse cycle is $8,750.
Solution: Automated expiration alerts at 21 and 7 days before every active authorization. One staff member assigned to authorization renewal as a primary responsibility.
Why Are Aging Claims Left Untouched?
Problem: Denied claims enter the AR queue and wait. Staff is busy with current billing. By the time someone works the 90-day bucket, some claims are past timely filing.
Financial impact: For every $10,000 in claims that age past timely filing, 100% is permanently uncollectible.
Solution: Weekly AR review sorted by dollar amount and age. Non-negotiable follow-up rule: every denied claim over $150 is worked within 10 business days.
Why Are Denials Repeating Every Month?
Problem: A denial is worked and resolved. The same denial code appears again next month from the same payer. No root cause was fixed.
Financial impact: Recurring denials are solvable with one process change that a practice never makes because no one is tracking patterns.
Solution: Monthly denial trend report by CARC code and payer. Top 3 denial codes receive a documented root cause and a process change each month.
Every Revenue Leak Has a Fix. Here's Where They All Are.
The Behavioral Health Operations Playbook covers psychiatry coding, denial prevention, AR recovery, authorization management, and the KPI framework high-performing practices use to protect revenue.
Why Is Eligibility Verification Often Ignored?
Problem: Coverage is verified at intake and never again. A patient switches insurance. Coverage lapses. Three sessions are delivered before anyone notices.
Financial impact: At $175 per session, three sessions for one patient are $525. At scale, eligibility-related denials typically represent 5 to 10% of monthly claims.
Solution: Automated eligibility verification 48 hours before every scheduled appointment, not just at intake.
Why Are Providers Leaving CPT Revenue on the Table?
Problem: Combined med management and therapy visits are billed as standalone 99214 when 99214 + 90836 was the correct billing. The psychotherapy component is never captured.
Financial impact: At 10 combined visits per week, missing 90836 on each costs $80 to $120 per visit in uncaptured reimbursement. That is $800 to $1,200 per week, $41,600 to $62,400 annually per provider.
Solution: Quarterly coding audit: 15 combined visits per provider reviewed against documentation. Discrepancies become training.
Why Is KPI Tracking So Important?
Problem: Collections look stable from month to month. Under the surface, the denial rate is rising, days in AR are creeping up, and net collection rate is falling. None of this is visible without weekly KPI tracking.
Solution: Six KPIs reviewed weekly: clean claim rate, denial rate, FPRR, days in AR, net collection rate, and authorization approval rate. Trends surface problems before they become significant financial events.
How Can Psychiatry Practices Improve Billing Performance?
| Step | Action | Frequency | Owner |
|---|---|---|---|
| 1. Eligibility Verification | Automated real-time check 48 hours before every appointment | Per appointment | Front desk/billing |
| 2. Coding Audit | 15 claims per provider reviewed against documentation | Quarterly | RCM manager |
| 3. Authorization Management | Expiration alerts at 21 and 7 days; reauth submitted 14 days before end | Ongoing | Auth coordinator |
| 4. Claim Scrubbing | CPT-to-documentation match, modifier check, POS code review before submission | Per claim | Billing team |
| 5. Denial Management | Weekly denial report by CARC code; root cause assigned; rework within 10 days | Weekly | AR lead |
| 6. KPI Monitoring | Six core KPIs reviewed weekly; trends flagged at threshold crossings | Weekly | RCM manager |
| 7. Revenue Optimization Review | Identify under-coded visits, missed add-ons, and payer rate gaps quarterly | Quarterly | RCM director |
What Does a High-Performing Psychiatry Revenue Cycle Look Like?
- Patient Scheduling
↓ - Eligibility Verification (automated, 48 hours before visit)
↓ - Authorization Confirmed (before session; expiration tracked)
↓ - Clinical Documentation (E/M level documented; psychotherapy time recorded)
↓ - Coding (E/M level matched to complexity; add-ons captured; modifier 25 applied)
↓ - Claim Scrubbing (modifier, POS, NPI confirmed; clearinghouse submission)
↓ - Payment Posting (contracted rate vs. actual payment reconciled)
↓ - Denial Management (weekly queue; root cause tracking; 10-day rework rule)
↓ - Revenue Reporting (KPI dashboard; trend analysis; optimization review)
Each stage has a defined owner, a quality check, and a standard. When any stage is unclear or inconsistently executed, revenue leaks.
Your Billing Performance Is a Revenue Strategy Decision.
BehavioralProz helps psychiatry practices optimize billing performance, reduce denials, and recover revenue from the gaps that clinical volume alone cannot close.
Frequently Asked Questions
How does billing impact psychiatry revenue?
Billing accuracy controls the portion of care delivered that actually comes back as collections. Coding errors, authorization expirations, MBHO routing errors, and unworked denials all strip collections from your revenue without showing up on the month-over-month revenue totals until a chunk of loss has been sustained.
Why do psychiatry claims get denied?
The most common causes are missing modifier 25 on E/M plus add-on claim combinations, MBHO carve-out routing errors, expired authorizations, and telepsychiatry modifier and POS code mistakes.
What is the biggest cause of revenue leakage in psychiatry practices?
Under-coding combined med management and therapy visits specifically not billing the psychotherapy add-on codes (90833, 90836, 90838) alongside E/M codes is the most consistent and most silent revenue leak across psychiatry practices.
How can psychiatry practices increase collections?
Conduct quarterly coding audits; Automate eligibility checks before EACH appointment; Manage authorization expiration with 21-day and 7-day notifications; Analyze monthly denial trends by CARC code to identify and fix the root issues instead of trying to fix individual denied claims.
What KPIs should psychiatry practices monitor?
Clean claim rate (target 95%+), denial rate (target under 5%), days in AR (target under 35), net collection rate (target 95%+), first-pass resolution rate (target 90%+), and authorization approval rate (target 85%+).
How important is credentialing for psychiatry billing?
Credentialing dictates whether a claim can even get paid. Delays in CAQH completion, MBHO carve-outs that haven’t been enrolled in, and new providers whose payer enrollment has not yet been completed result in uncompensated visits that usually can’t be retrospectively collected.