Table of Contents
Before there was something called prior authorization, it used to be a useful little utilization management tool. But for behavioral health providers, prior authorization is one of the heaviest lifts and biggest claim denial generators in the entire specialty.
Just the other day in a behavioral health online community, a therapist posted: “We had a patient in IOP for three weeks. We thought authorization was established…it was not. Payer retro denied all three weeks of care. Daily sessions denied retroactively. Couldn’t even appeal with success because we didn’t even wait until we validated authorization and provided care.”
Sound familiar? Well, it happens every day. The only difference between successful providers who excel at prior authorization and the ones that don’t comes down to the payers and the workflow they have established.
Why Do Behavioral Health Practices Struggle With Prior Authorization?
Here are the operational breakdowns I see consistently when I lurk in online forums and community pages where behavioral health billing is discussed:
- Manual tracking systems: Authorizations tracked in spreadsheets or individual clinician calendars, not a centralized system with alerts.
- No concurrent review calendar: PHP and IOP programs know concurrent review is required but have no system to track upcoming review dates.
- MBHO confusion: Authorization requests submitted to the base commercial payer when the behavioral health benefit is managed by a separate MBHO denial guaranteed.
- Documentation not matched to payer criteria: Medical necessity documentation written in clinical language that doesn’t map to the payer’s specific LOC criteria.
- Reauthorization treated as an afterthought: Initial authorization obtained; reauthorization missed because no alert system exists.
- Staff turnover: The staff member who “knows” the authorization status for each patient leaves; institutional knowledge leaves with them.
Authorization Lapses Are Costing You Every Day They Go Untracked.
BehavioralProz manages prior authorization requests, concurrent review tracking, reauthorization deadlines, and appeal workflows for behavioral health practices at every size.
Which Behavioral Health Services Typically Require Prior Authorization?
| Service Type | Authorization Required? | Common Documentation Needed | Common Payer Challenges |
|---|---|---|---|
| Outpatient therapy (standard) | Varies, often after session 8 to 20 | Diagnosis, treatment plan, progress notes | Some plans allow initial sessions without auth |
| Psychiatry / med management | Sometimes particularly Medicaid MCOs | Diagnostic evaluation, treatment plan | MBHO may require separate auth from commercial plan |
| Psychological testing | Usually yes | Referral, clinical justification, testing plan | Strict criteria; preauthorization often required |
| IOP (ASAM 2.1) | Yes | ASAM assessment, treatment plan, progress notes | Short auth windows; concurrent review every 3 to 7 days |
| PHP (ASAM 2.5) | Yes | ASAM assessment, physician oversight notes | High documentation scrutiny; frequent concurrent review |
| Residential (ASAM 3.1 to 3.7) | Yes before admission | ASAM assessment, admission history, treatment plan | Retroactive auth rarely approved; admission auth required |
| ABA therapy | Yes | Autism diagnosis, BCBA-prepared treatment plan, BCBA assessment | Separate auth for assessment vs. treatment; BCBA supervision required |
| Substance abuse treatment | Yes | ASAM assessment, LOC justification, treatment plan | Strict LOC criteria; proprietary payer criteria in addition to ASAM |
| Telehealth behavioral health | Varies | Same as in-person plus modality confirmation | Some plans require separate auth for telehealth modality |
What Are the Most Common Prior Authorization Mistakes?
Why Do Practices Submit Incomplete Authorization Requests?
What happens: A payer returns an authorization request incomplete. The process restarts. Treatment is delayed or delivered without auth.
Why it occurs: No pre-submission documentation checklist. Requests assembled from memory rather than from a confirmed payer requirement list.
Revenue impact: Treatment delays, patient cancellations, and retroactive denials when treatment begins before auth is confirmed.
How to avoid it: Build a payer-specific documentation checklist for every service type you bill. Verify requirements annually; payers update criteria regularly.
Why Are Medical Necessity Documents Often Rejected?
What happens: An authorization request includes a treatment plan and diagnosis. The payer denies for insufficient medical necessity. The documentation did not speak to the payer’s specific LOC criteria.
Why it occurs: Clinical staff write documentation in clinical language. Payer reviewers evaluate against proprietary criteria that do not use the same language.
How to avoid it: Write medical necessity documentation to the payer’s published criteria using their language, addressing their specific dimensions. For ASAM-based payers, the ASAM six-dimension framework should be explicitly addressed.
Why Do Authorizations Expire Before Treatment Ends?
What happens: A patient is in treatment. The authorization expires. No one catches it until a claim denies retroactively for dates after the expiration.
Why it occurs: No expiration alert system. Auth end dates exist somewhere in a spreadsheet or in the EHR, but no one is looking at them systematically.
Revenue impact: Every claim after the expiration date is denied. Recovery requires retro auth requests, which most payers deny.
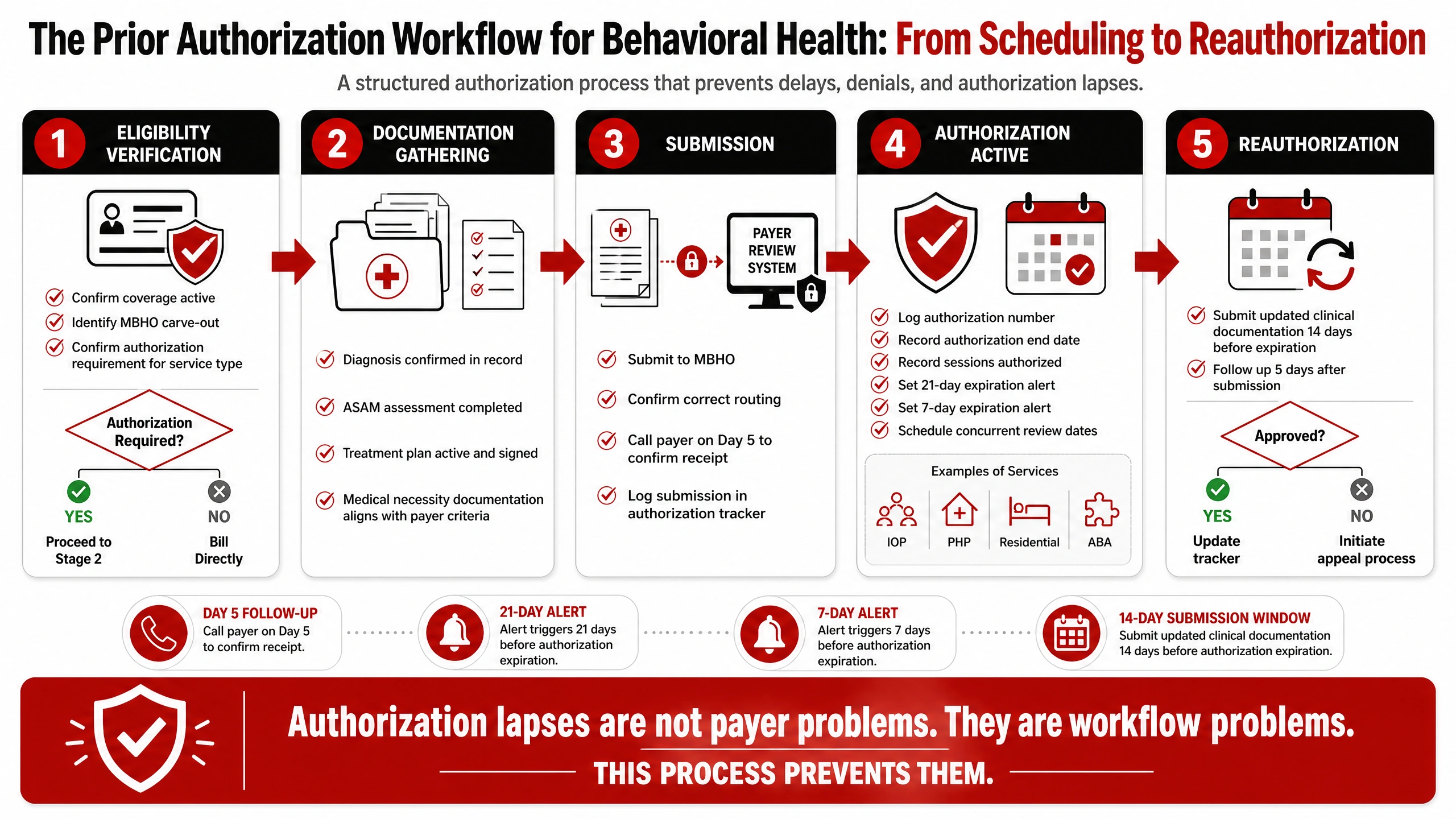
How to avoid it: Automated expiration alerts at 21 days and 7 days before every active auth end date. One assigned staff member owns reauthorization for each service line.
The Authorization Workflow Is One Chapter. Your Operations Playbook Covers the Rest.
The Behavioral Health Operations Playbook includes authorization tracking frameworks, denial prevention tools, RCM KPI benchmarks, and operational checklists built for behavioral health practices.
Why Do Practices Miss Reauthorization Deadlines?
What happens: Reauthorization requires submitting updated clinical documentation before the current authorization expires. The deadline is missed by one week. Treatment continues. Every session after the expiration is denied.
Why it occurs: Reauthorization is treated as a future task that gets pushed back. The concurrent review calendar exists only in someone’s memory.
How to avoid it: Build a reauthorization calendar with 30-day and 14-day alerts before every expiration. Submit reauthorization requests at least 14 days before expiration to allow payer processing time.
Why Do Payers Deny Behavioral Health Services After Approval?
What happens: Authorization was obtained. Sessions were delivered. The payer conducts a post-service audit. Documentation does not support the authorized level of care. Claims are denied retroactively.
Why it occurs: The authorization was approved based on the initial request. The ongoing clinical documentation did not maintain the medical necessity standard the payer’s concurrent reviewers expected.
How to avoid it: Every progress note for authorized services should reflect ASAM dimensional criteria, observable clinical progress or documented barriers, and active justification for the current level of care. Vague session notes, copied forward, or disconnected from LOC criteria create retroactive audit risk.
RELATED READING


Why Is Authorization Tracking So Difficult?
What happens: A practice has 40 active authorized patients across three payers. Each payer has different auth windows. Some require concurrent review every 3 days; others every 14 days. The practice tracks this in a shared spreadsheet that gets updated inconsistently.
Why it occurs: Authorization tracking at volume requires a systematic solution. Spreadsheets work at 10 patients. They fail at 40.
How to avoid it: Implement an authorization tracking system either within your EHR (if it supports this) or a dedicated tracker with automated alert functionality. Each record should contain: auth number, payer, MBHO, service type, start date, end date, sessions authorized, sessions used, next review date, and owner.
Why Do Staff Members Spend Hours Following Up?
What happens: An authorization request is submitted. After two weeks, there is no response. A staff member spends 40 minutes on hold to confirm receipt. This happens with every new authorization, across every active payer.
Why it occurs: No structured follow-up cadence. Authorization follow-up competes with every other administrative task.
Revenue impact: Staff time cost is real, and the authorization delay translates directly to delayed billing.
How to avoid it: Build a follow-up cadence: call payer at day 5 after submission to confirm receipt. Call at day 10 for status. Escalate to provider relations at day 15 if no determination. Document every call with date, representative name, and reference number.
How Can Practices Build a Better Prior Authorization Workflow?
How Does Prior Authorization Affect Revenue Cycle Performance?
Billing challenges aren’t the only side effect. Authorization failures are contagious throughout the revenue cycle.
- Delayed reimbursement: When you provide treatment without authorization confirmation, the claim goes on hold until authorized.
- Increased AR aging: Denial based on authorization creates the claim in your A/R and requires additional legwork to be resubmitted for payment.
- Revenue loss: When retroactive authorizations were declined, you don’t collect for the services that the patient was provided.
- Staff productivity: When manually keeping up with authorizations and denials requires about 10 to 20+ hours a week for average sized practices.
- Patient cancellations: Unresolved auth issues cause the provider to delay treatment, which usually leads the patient to find care elsewhere.
- Collections impact: Your net collection rate suffers when claims with denials due to authorizations are unworked beyond timely filing deadlines.
What Technologies Can Help Automate Prior Authorization?
- EHR-integrated auth tracking: Systems like Netsmart and AdvancedMD include authorization modules with expiration alerts; configure these before relying on manual tracking.
- Clearinghouse authorization tools: Availity and Waystar both offer authorization submission and status tracking within the same platform used for eligibility and claims.
- AI-assisted prior auth platforms: Tools purpose-built for authorization management (Olive, Rhyme, Waystar Auth) use AI to pre-populate requests and predict approval likelihood.
- Workflow automation: Rules-based automation can trigger documentation requests, expiration alerts, and reauthorization tasks without manual scheduling.
- EHR documentation prompts: ASAM-dimensional documentation prompts embedded in progress note templates ensure notes are written to payer expectations from the start.
6 Steps Practices Do When Prior Authorization Is Denied
Step 1: Read the denial letter. This determines if your authorization was denied based on medical necessity, inadequate info, or LOC criteria.
Step 2: Request the specific criteria used to make the determination. The payer is required by the MHPAEA to share the actual criteria they use in their denial.
Step 3: Prepare the appeal. Include updated clinical documentation written to the payer’s specific criteria. Address every dimension the payer cited in the denial.
Step 4: Request a peer-to-peer review. The treating provider or BCBA gets directly on the line with the payer’s medical reviewer to go over the case, and peer-to-peers generally are approved more frequently.
Step 5: If the peer-to-peer is denied, escalate to an external independent review organization (IRO). Both commercial payers and Medicaid programs offer IRO appeals.
Step 6: If the denial pattern appears inconsistent with equivalent medical/surgical coverage, file an MHPAEA parity complaint with your state insurance commissioner. Document the pattern across multiple patients.
Stop Losing Revenue to Authorization Failures You Could Have Prevented.
BehavioralProz builds authorization management workflows that prevent lapses, reduce denials, and recover retroactive auth revenue for behavioral health programs.
Frequently Asked Questions
What is prior authorization in behavioral health?
It is a payer requirement that an authorizing form be submitted and approved before a particular behavioral health service is rendered. When that prior authorization is not in place, the service will be denied for a member in any panel network.
Does therapy require prior authorization?
It depends on the payer and the number of sessions. Many commercial plans allow an initial number of sessions (typically 8 to 20) without authorization but require prior auth for continued treatment. Confirm requirements with each payer at benefits verification.
How long does prior authorization take for behavioral health?
Most payers process initial authorization requests within 5 to 10 business days. Urgent requests (for PHP or residential admission) can often be expedited to 24 to 72 hours. Delays are common when documentation is incomplete.
Can a claim be denied even if authorization was obtained?
Yes. If the clinical documentation for delivered services does not match the authorized level of care, payers can retroactively deny on a post-service audit. Authorization approval does not guarantee claim payment; the documentation must continue to support the authorized services throughout treatment.
What happens if authorization expires during treatment?
Every claim for services delivered after the expiration date will be denied. Retroactive authorization is rarely approved. Practices must initiate reauthorization at least 14 days before expiration.
How can behavioral health practices reduce authorization denials?
By matching documentation to payer-specific LOC criteria, building expiration tracking with automated alerts, submitting reauthorization at least 14 days in advance, and requesting peer-to-peer review for medical necessity denials before accepting them.