Table of Contents
A billing manager at a behavioral health group practice shared in an RCM forum: “We have $180,000 in denied claims sitting in AR right now. Some are 45 days old. Some are 120 days old. Some are probably past timely filing already. We know the denials happened. We just don’t have the bandwidth to work all of them.”
That’s not a billing failure. That’s a denial management system failure, and it’s more common than most practices admit. Behavioral health claim denials follow predictable patterns. The same 10 denial types generate the overwhelming majority of lost revenue across every specialty in this field. This guide breaks down all 10, with the root cause, the payer trigger, and the exact fix for each.
Why Do Behavioral Health Claims Get Denied More Than Other Medical Specialties?
Behavioral health has a structurally higher denial rate than most medical specialties, for three documented reasons:
- MBHO carve-out complexity: Most commercial payers separate behavioral health into managed behavioral health organizations (Optum, Carelon, Magellan). Every carve-out is a separate enrollment, separate auth system, and separate claims routing requirement. One routing error = denial.
- Authorization burden: Behavioral health services face prior authorization requirements at higher rates than equivalent medical/surgical services, a documented parity disparity. More auths = more auth-related denials.
- Documentation specificity requirements: Mental health and substance abuse services require documentation standards (ASAM criteria, time-based CPT documentation, concurrent review notes) that many practices aren’t consistently meeting.
The result: a typical behavioral health practice runs a denial rate of 7–15%. Best-in-class is below 3%. The gap between those numbers represents recoverable revenue, if the right processes are in place.
Your Denied Claims Are Aging Right Now. Every Day Matters.
Most behavioral health practices have 10–20% of their recoverable revenue sitting in denied claims, not because the claims were wrong, but because nobody worked them. BehavioralProz finds the patterns, fixes the root causes, and recovers the revenue before the window closes.
What Is the Real Financial Cost of Behavioral Health Claim Denials?
Quick math: A practice billing $600K/year with a 10% denial rate has $60,000 in denied claims per year. If 40% of those are never worked or recovered, that’s $24,000 in permanently lost revenue annually, not from wrong treatment, not from payer policy, but from process failures that repeat monthly.
At scale, a 20-provider group billing $3M/year, the same math produces $120,000 in annual unrecovered revenue. Most practices don’t track this number. They see collections and assume billing is working.
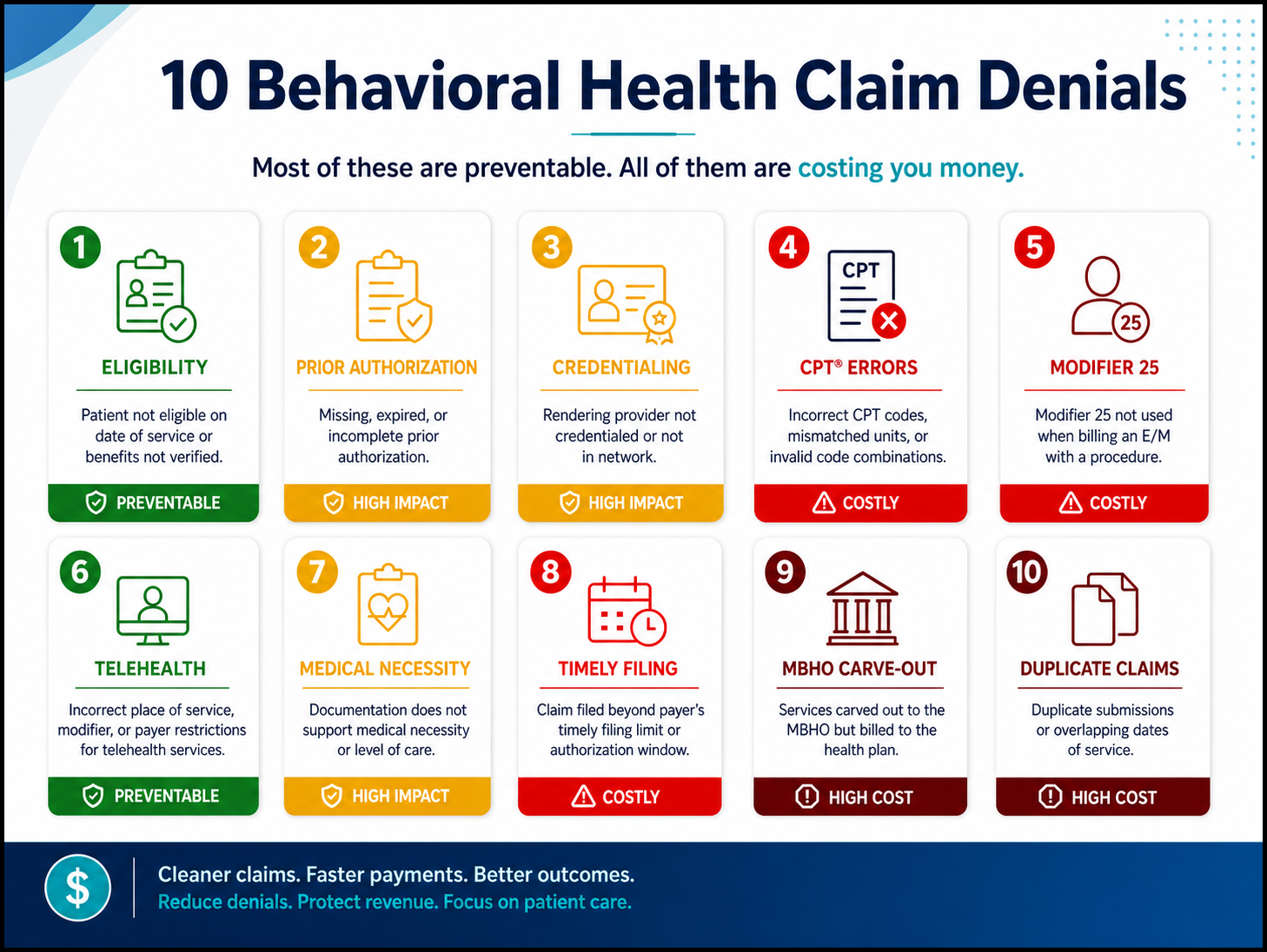
10 Common Behavioral Health Claim Denials
Claim denials are a frequent headache for behavioral health providers, but most follow familiar patterns that can be fixed with targeted process improvements. From missing authorizations to incorrect CPT codes and improper telehealth modifiers, the denials below represent the top reasons claims fail. So, here are the most common denials:
- Eligibility Verification Failures
- Prior Authorization Denials
- Credentialing-Related Denials
- Behavioral Health CPT Coding Errors
- Missing Modifier 25
- Telehealth Modifier and POS Errors
- Medical Necessity Denials
- Timely Filing Violations
- MBHO Carve-Out Routing Errors
- Duplicate Claim Denials
#1: Why Do Eligibility Verification Failures Cause So Many Denials?
What happens: A patient’s insurance lapsed, changed plans, or hit a benefit limit, and the practice didn’t catch it before billing. The claim is submitted, denied (CO-27: expenses incurred after coverage terminated, or CO-22: coordination of benefits), and the practice is left chasing either the payer or the patient.
Why it keeps happening: Most practices verify eligibility at intake, once. Insurance changes constantly. Patients get new jobs, switch Medicaid plans, age off parents’ coverage, hit annual benefit caps, and forget to notify their providers.
The fix: Run automated eligibility verification through your clearinghouse (Availity, Waystar) for every active patient, every week. Flag any change before the appointment. Document every verification with a reference number.
#2: Why Do Prior Authorization Denials Keep Happening Even When You Think You're Covered?
What happens: A service was provided and billed, but the authorization on file was expired, covered a different level of care, or was issued for a different provider. The claim denies retroactively.
Why it keeps happening: Authorization management is tracked informally- a sticky note, a shared calendar, a biller who “knows” the expiration dates. When volume increases, or staff turns over, the system collapses.
The fix: Build authorization expiration alerts into your workflow at 21 days and 7 days before expiration. Assign ownership: one person or role is accountable for every active authorization in the system. Nothing renews by accident.
#3: Why Do Credentialing-Related Denials Go Undetected for So Long?
What happens: A provider is credentialed with Aetna, but behavioral health is carved out to Evernorth. Claims submit, appear to go through, and then come back denied weeks later: “Provider not enrolled.” Or a CAQH profile expires silently, suspending enrollment with every payer simultaneously.
Why it keeps happening: Credentialing is treated as a one-time event, not an ongoing maintenance function. CAQH re-attestation every 120 days, MBHO carve-out enrollment separate from commercial plan enrollment, and provider specialty updates are rarely tracked systematically.
The fix: Maintain a credentialing status tracker for every provider, payer, enrollment date, effective date, CAQH attestation date, and next review date. Review it monthly. Flag anything expiring within 30 days.
#4: Why Do Behavioral Health CPT Coding Errors Trigger Systematic Denials?
What happens: The practice bills 90837 for all sessions regardless of documented time. Or it bills CPT codes to a Medicaid payer that requires HCPCS H-codes. Or a SUD program bills H0015 to a commercial plan that requires S9480. CO-4 (procedure not covered), every time, on every claim, for every affected payer.
Why it keeps happening: No payer-specific billing reference exists. Billers apply the same code set to every payer out of habit. No quarterly coding audit catches the pattern.
The fix: Build a payer-specific code reference for your top 10 payers. Run a quarterly coding audit, 10 claims per clinician, compared against session notes and payer requirements. The pattern surfaces within one audit cycle.
#5: Why Does Missing Modifier 25 Kill Psychiatry and Behavioral Health Claims?
What happens: A psychiatrist or PMHNP bills 99214 + 90836 (E/M + psychotherapy add-on) without appending modifier 25 to the E/M code. The payer bundles the E/M into the add-on and denies the E/M with CO-97 (payment adjusted, previously processed).
Why it keeps happening: Billers new to psychiatry billing don’t know modifier 25 is required when billing E/M + add-on together. It’s not prompted by most practice management systems automatically.
The fix: Add modifier 25 as a required field in your billing workflow for any claim that includes an E/M code paired with a same-day procedure or add-on code. Make it impossible to submit a combined visit without it.
#6: Why Do Telehealth Modifier and POS Errors Still Generate Denials in 2026?
What happens: A telehealth session is submitted with POS 11 (office) instead of POS 10 (patient at home). Or modifier GT is used when the payer now requires modifier 95. The claim either denies or reimburses at the wrong rate.
Why it keeps happening: Telehealth billing rules changed multiple times between 2020 and 2025. Practices that updated their workflows once, but not continuously, are often running outdated modifier and POS combinations.
The fix: Maintain a payer-specific telehealth modifier reference (95 vs GT, POS 10 vs POS 02) updated quarterly. Review telehealth billing guidance from your top 5 payers at the start of each calendar year.
#7: Why Do Medical Necessity Denials Hit Behavioral Health Harder Than Other Specialties?
What happens: The payer’s concurrent reviewer determines the patient no longer meets clinical criteria for the authorized level of care. The authorization lapses. All subsequent claims are denied: CO-11 (diagnosis inconsistent with procedure) or equivalent medical necessity code.
Why it keeps happening: Clinical documentation doesn’t reflect ASAM criteria or the payer’s proprietary level-of-care criteria. Notes are vague, copy-forwarded, or don’t establish why the patient needs continued treatment at this level.
The fix: Build ASAM dimensional documentation prompts directly into your EHR note templates. Every note for IOP, PHP, residential, or high-frequency outpatient must answer: Why does this patient need this specific level of care today? Make the clinical justification structural, not optional.
Recovery path: Medical necessity denials are among the most appealable denial types. Submit an appeal with ASAM-based clinical documentation, the payer’s own coverage criteria (quote the applicable section), and a request for peer-to-peer review on high-dollar claims.
Medical Necessity Denials Are Opinions. They're Appealable.
Most medical necessity denials are overturned on first appeal when the right clinical documentation is submitted. BehavioralProz handles appeals, peer-to-peer reviews, and parity-based escalations for behavioral health practices at every level of care.
#8: Why Do Timely Filing Violations Permanently Destroy Revenue?
What happens: A claim was denied, placed in a work queue, and sat there for 120 days. When the biller finally attempts to resubmit or appeal, the payer’s timely filing window has closed. The revenue is gone, permanently, regardless of clinical or billing accuracy.
Why it keeps happening: Denial queues are worked reactively, when someone “has time” rather than on a defined schedule. High-volume practices with understaffed billing teams lose track of aging claims until it’s too late.
The fix: Set a non-negotiable rule: every denial over $100 receives a follow-up within 10 business days. Every denied claim is re-evaluated at 30, 45, and 60 days. Any claim approaching the 75-day mark gets escalated immediately.
#9: Why Do MBHO Carve-Out Routing Errors Cause Claims to Disappear?
What happens: A behavioral health claim is submitted to the base commercial payer, but the patient’s behavioral health benefit is carved out to Optum Behavioral Health, Carelon, or Magellan. The base payer doesn’t adjudicate it. No denial is generated. The claim just sits, no payment, no denial, no action trigger.
Why it keeps happening: Benefits verification confirmed insurance coverage, but didn’t confirm whether behavioral health was carved out. The practice has no systematic MBHO check at intake.
The fix: Add an explicit behavioral health carve-out check to your benefits verification workflow. Ask at every verification: “Is behavioral health managed by a separate organization? If so, what is the payer ID for behavioral health claims?” Document the answer.
#10: Why Do Duplicate Claim Denials Happen After Resubmission?
What happens: A claim is denied. The biller resubmits it as a new claim without the original claim number (ICN/TCN). The payer adjudicates both and denies the second as a duplicate with CO-18.
Why it keeps happening: Billing staff unfamiliar with corrected claim submission protocols resubmit denials as new claims by default. The original claim number, required for corrected submissions, is never entered.
The fix: Train billing staff on claim frequency codes. A corrected claim (frequency code 7) requires the original claim’s ICN/TCN in the appropriate field. A new claim (frequency code 1) is used only for claims with no prior submission. Resubmitting without the original claim number is not a correction; it’s a duplicate.
What Is the Master Denial Prevention Framework for Behavioral Health Practices?
The Denial Prevention Master Table
| Denial Type | Primary Cause | Prevention Action | Recovery Path |
|---|---|---|---|
| Eligibility failure | Lapsed coverage, plan change | Weekly automated eligibility verification | Bill patient; verify new coverage |
| Authorization denial | Expired or missing auth | 21-day expiration alerts; ownership assigned | Retro auth request; peer-to-peer |
| Credentialing denial | MBHO not enrolled; CAQH expired | Monthly credentialing tracker review | Expedited enrollment; retro billing when allowed |
| CPT coding error | Wrong code for payer | Payer-specific code reference; quarterly audit | Corrected claim with correct code |
| Missing modifier 25 | Habit; no workflow prompt | Required modifier field in billing system | Corrected claim with modifier added |
| Telehealth modifier error | Outdated modifier/POS | Annual payer telehealth review | Corrected claim with correct modifier/POS |
| Medical necessity denial | Weak documentation | ASAM prompts in EHR templates | Written appeal + peer-to-peer |
| Timely filing | Denial queue not worked | 10-day follow-up rule; weekly aging review | Escalate immediately; check window |
| MBHO routing error | Carve-out not confirmed | BH carve-out check in benefits verification | Reroute claim; confirm payer ID |
| Duplicate claim | Wrong resubmission type | Corrected claim training; ICN/TCN required | No recovery; avoid with correct process |
Prevention Workflow Checklist
Front-end (before service):
- [ ] Eligibility verified this week for every scheduled patient
- [ ] Behavioral health carve-out confirmed; MBHO payer ID documented
- [ ] Authorization active; expiration date tracked
At documentation:
- [ ] Session time documented (start/stop) for time-based CPT codes
- [ ] Clinical specificity present; no copy-forward
- [ ] Medical necessity language supports level of care billed
At submission (within 3 business days):
- [ ] Correct CPT code for this payer confirmed
- [ ] Required modifiers applied (modifier 25, 95/GT for telehealth)
- [ ] Correct POS code (10 for home telehealth, 11 for in-person)
- [ ] Claim routed to correct entity (MBHO vs. base payer)
Weekly denial management:
- [ ] Denial report pulled; sorted by dollar amount and age
- [ ] Every denial over $100 assigned for follow-up within 10 days
- [ ] Any claim approaching 60 days escalated immediately
Denial Prevention Is Operations. Your Playbook Is Already Written.
The Behavioral Health Operations Playbook covers denial prevention workflows, authorization management, coding accuracy, RCM KPIs, and clean claim processes- everything a behavioral health practice needs to stop leaving revenue on the table.
Frequently Asked Questions
What is the most common behavioral health claim denial?
Missing or expired prior authorization is the top cause, followed by eligibility verification failures and MBHO carve-out routing errors; all three are preventable with front-end workflow improvements.
How can behavioral health providers reduce claim denials?
Verify eligibility weekly, track authorization expirations proactively, confirm MBHO carve-out routing at intake, use payer-specific CPT references, and apply required modifiers (25, 95) before submission.
What is a medical necessity denial in behavioral health?
A payer determination that the service billed doesn’t meet clinical criteria for the level of care provided. Most are overturned on appeal when supported by ASAM-based clinical documentation and peer-to-peer review.
Can denied behavioral health claims be recovered?
Yes, most denials, except for timely filing violations, are recoverable through corrected claim resubmission or formal appeal. Medical necessity, modifier errors, and coding mistakes have high overturn rates with correct documentation.
How long do behavioral health providers have to appeal a denial?
Most payers allow 30–180 days from the denial date to submit a first-level appeal. Timelines vary by payer; confirm per payer’s remittance advice. Failing to appeal within this window makes the denial permanent.
What is an MBHO carve-out and why does it cause denials?
A managed behavioral health organization (MBHO) carve-out means the commercial payer has routed behavioral health benefits to a separate entity (Optum, Carelon, Magellan). Claims submitted to the base payer instead of the MBHO are either denied or never adjudicated.
What is the difference between a rejected claim and a denied claim?
A rejected claim failed technical edits before reaching the payer; it was never adjudicated and requires correction and resubmission. A denied claim entered the system and was adjudicated but not paid, with a documented denial reason code.
What is modifier 25 and when is it required in behavioral health billing?
Modifier 25 is appended to an E/M code to indicate that it is a separately identifiable service from a procedure or an add-on code billed on the same day. In psychiatry, it’s required when billing 99213–99215 with a psychotherapy add-on (90833, 90836, 90838).
What is timely filing in behavioral health billing?
Timely filing is the payer’s deadline for submitting a claim from the date of service, typically 90–180 days. Claims submitted after this window are permanently denied with no recourse, regardless of accuracy.