Table of Contents
“We’ve got $94k in denied claims sitting here at the moment,” an ABA clinic director posted to a BCBA billing forum. “Some of them are 60-day, some 90-day. We just realized our RBT’s NPI number wasn’t added to one of our large payers, so we didn’t have a clue about the four months of denied claims from her.”
That is not an isolated example.
In fact, ABA billing has more potential for claim denials than just about any other behavioral health niche. You have to account for multiple provider levels. Tight author/timeframes. Specific documentation rules per payer for supervision. State-specific rules under Medicaid, etc. It’s an amazing process for generating retroactive denials whenever anyone misses any of the many due dates within concurrent review cycles.
You can avoid the vast majority of these denials if you know where to look before submission.
Why Do ABA Claims Get Denied So Frequently?
The complexity in ABA billing is systemic, not an add-on complication. There are 3 underlying reasons ABA denial rates are significantly higher than in other specialties:
- Multiple provider levels: BCBA, BCaBA, RBT, and behavioral technicians all submit claims based on their own individual NPI number and require specific codes and modifier documentation based on the individual payer’s supervision documentation policies
- Concurrent authorization cycles: ABA services necessitate re-authorization every 30-180 days per payer; this leaves all currently active patients at risk for retro-denied services when these cycle gaps are identified
- Payer-defined coding: Some payers require CPT codes, while others use HCPCS H-codes; some payers require both codes for different types of ABA services. Billing the wrong codes for a payer results in claim Denial CO-4
Your ABA Denial Rate Is a Revenue Strategy Problem.
Most ABA practices are losing 15 to 22% of claims to preventable denials. BehavioralProz provides ABA-specific billing, authorization management, denial recovery, and coding audits built for autism clinics, not generalist medical practices.
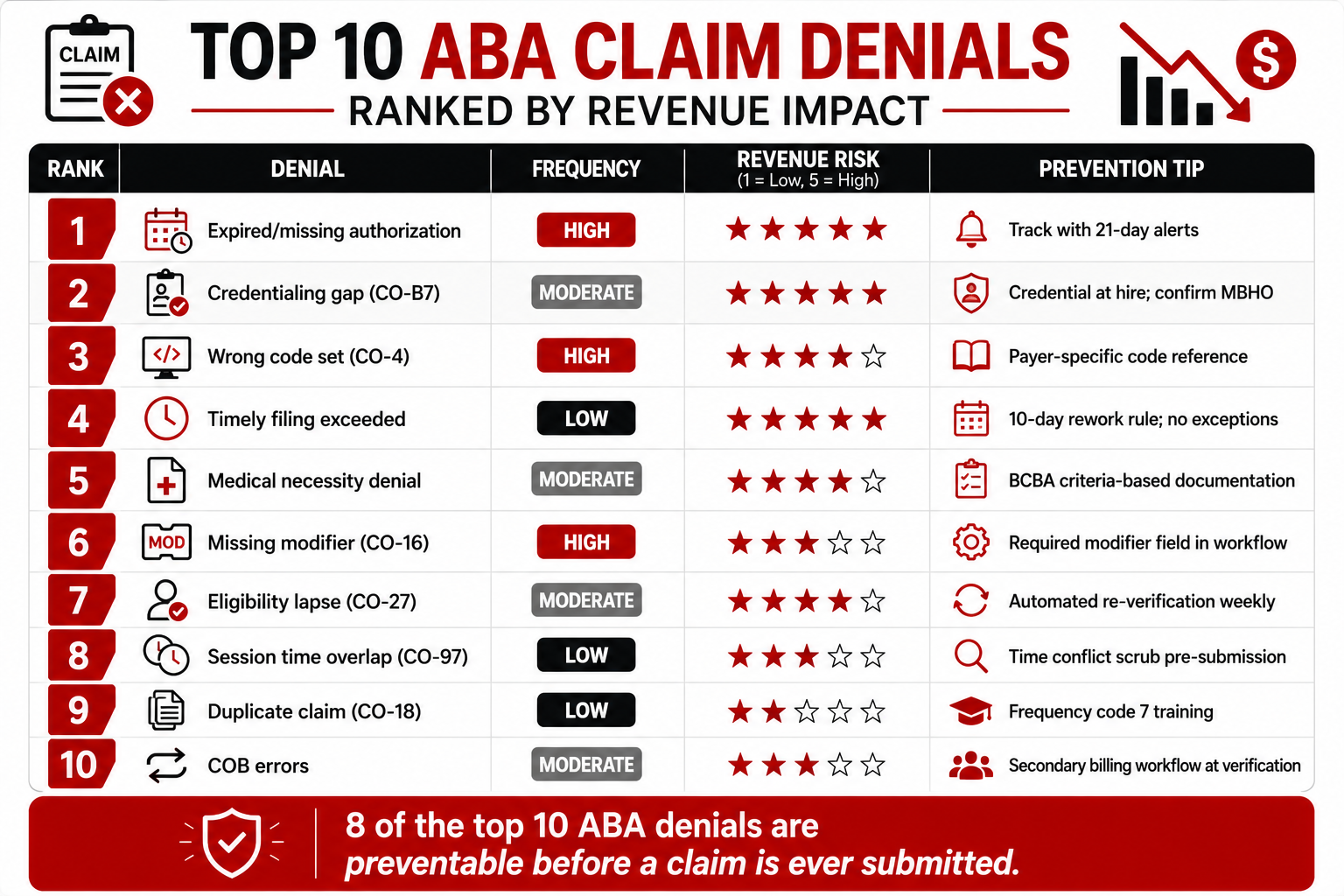
Top 10 Reasons ABA Claims Get Denied
ABA billing fails in predictable places. The same denial codes appear on the same claim types from the same payers, month after month, because the root cause was never fixed. Understanding exactly where and why each denial originates is the first step to stopping it permanently.
Here are the 10 most common reasons ABA claims get denied and what to do about each one:
- Prior Authorization Missing or Expired
- Incorrect ABA CPT Codes
- Missing Required Modifiers
- Documentation Fails Medical Necessity
- Eligibility Verification Errors
- Timely Filing Limits
- Credentialing Delays and Payment Blocks
- Duplicate Claim Rejections
- Session Time Conflicts
- Coordination of Benefits Errors
#1 Prior Authorization Missing or Expired
Why it happens: Authorization obtained at admission; no tracking system for expiration or concurrent review deadlines. A review date is missed by one week.
Revenue impact: Every claim after the expiration date is denied retroactively. For a caseload of 25 patients at $200 per session, one week of lapsed authorization is $5,000 in at-risk claims.
Prevention: Automated expiration alerts at 21 and 7 days. One assigned staff member owns every active authorization renewal. Submit reauth requests 14 days before expiration minimum.
#2 Incorrect ABA CPT Codes
Why it happens: Billing staff submit H2019 (Medicaid) to a commercial payer that requires 97153. Or they bill 97155 (BCBA protocol modification) for sessions where only an RBT was present. Or 97153 and 97155 are billed as standalone codes rather than with the correct time-unit calculation.
Revenue impact: CO-4 denials on every claim using the wrong code systematically, month after month, until someone identifies the pattern.
Prevention: Maintain a payer-specific code reference for your top 10 payers. Run a quarterly coding audit of 15 claims per provider compared against session notes and payer requirements.
#3 Missing Required Modifiers
Why it happens: ABA modifiers (HN, HO, HP for provider education level; HQ for group; 95 or GT for telehealth) vary by payer and are frequently omitted or applied incorrectly. Some Medicaid programs require U-series modifiers that billing staff are unaware of.
Revenue impact: CO-16 denials (missing required information) across all affected claims. Modifier 95 missing from telehealth ABA sessions generates systematic denials from commercial payers.
Prevention: Build modifier requirements into your billing workflow as required fields. Payer-specific modifier reference reviewed quarterly. No claim is submitted without modifier validation.
#4 Documentation Fails Medical Necessity
Why it happens: Progress notes do not address the payer’s specific medical necessity criteria. Notes are vague, copied forward, or disconnected from treatment plan goals. BCBA supervision ratios are not documented per session.
Revenue impact: Post-service audits recover payments already made. Concurrent review denials retroactively pull authorization mid-treatment.
Prevention: Build medical necessity language prompts into session note templates. Every note must address: presenting behavior, intervention delivered, patient response, and progress toward treatment plan goals. BCBA supervision type and ratio are documented on every applicable session.
#5 Eligibility Verification Errors
Why it happens: Coverage verified at intake, never again. Patient switches Medicaid MCO. Plan year resets. ABA benefit carved to a separate payer entity not identified at verification.
Revenue impact: CO-27 (expenses incurred after coverage terminated) or CO-4 (procedure not covered by payer) across every session delivered after the coverage change.
Prevention: Automated real-time eligibility verification before every appointment. ABA benefit verified separately from general behavioral health benefit. ABA is frequently carved to a different entity. Behavioral health RCM analytics platforms can automate this check across large patient volumes.


#6 Timely Filing Limits
Why it happens: A claim is denied, placed in a queue, and nobody works on it. Timely filing limits (typically 90 to 180 days from the date of service) pass. The claim is permanently uncollectable.
Revenue impact: 100% of the claim value is lost. No appeal is possible. For a $94,000 denial backlog like the one described above, even 30% aging past filing limits is $28,000 permanently gone.
Prevention: Every denied claim over $150 was worked within 10 business days. Weekly AR aging review. Any claim approaching 60 days is flagged for immediate escalation.
#7 Credentialing Delays and Payment Blocks
Why it happens: A new RBT starts seeing patients before their NPI is enrolled with the payer. A BCBA is enrolled with the commercial plan but not with the MBHO (Optum BH, Carelon, Magellan) managing the ABA benefit. CAQH profile lapses mid-credentialing cycle.
Revenue impact: CO-B7 (provider not eligible on date of service) across every claim from the unenrolled provider retroactively, for the entire unenrolled period.
Prevention: Begin credentialing applications at hire. Confirm MBHO carve-out enrollment separately from commercial plan enrollment. CAQH re-attestation alerts at 90 and 30 days before expiration.
#8 Duplicate Claim Rejections
Why it happens: A claim is denied. The biller resubmits it as a new claim without the original ICN/TCN. The payer receives two claims for the same service and denies the second as a duplicate (CO-18).
Revenue impact: The resubmission window is consumed; the corrected claim may need to be resubmitted again, compressing the remaining timely filing window.
Prevention: Train billing staff on frequency code 7 (corrected claim) vs. frequency code 1 (new claim). Corrected claims require the original claim ICN/TCN in the appropriate field. No duplicate submission without the root cause corrected first.
#9 Session Time Conflicts
Why it happens: Two services are billed for the same patient at overlapping times, for example, 97153 (RBT direct therapy) and 97155 (BCBA protocol modification) submitted with the same start and end time. Or a parent caregiver training session (97156) billed with the same time block as the patient’s direct therapy session.
Revenue impact: CO-97 (payment adjusted included in another service) or claim-level denial depending on payer rules.
Prevention: Document time blocks separately for concurrent services. 97153 and 97155 can be billed simultaneously but require separate time documentation. The billing system should flag time overlap conflicts before submission.
#10 Coordination of Benefits Errors
Why it happens: A patient has both commercial insurance and Medicaid. The primary claim is submitted, paid, and the secondary claim is either never submitted or submitted without the primary EOB attached. Some practices never bill secondary at all.
Revenue impact: Secondary insurance revenue is entirely uncaptured, often 10 to 20% of the patient’s per-session cost share.
Prevention: Confirm COB status at every benefits verification. Submit secondary claims within 30 days of primary adjudication. Attach the primary EOB to every secondary submission.
Same Denial Code. Every Month. It Is Time to Fix the Root Cause.
Recurring ABA denials are not payer problems. They are process problems. BehavioralProz identifies the pattern, corrects the workflow, and stops the denial before the next billing cycle.
Which Denial Reasons Cost ABA Practices the Most Money?
How Can ABA Practices Prevent Claim Denials Before Submission?
| Step | Action | Owner | Timing |
|---|---|---|---|
| 1. Eligibility Verification | Automated real-time check including ABA benefit and MBHO routing | Front desk/billing | 48 hours before the visit |
| 2. Authorization Validation | Confirm active auth; sessions remaining; upcoming expiration | Auth coordinator | Before every session |
| 3. Coding Review | CPT vs. H-code confirmed per payer; modifier requirements applied | Billing team | At claim generation |
| 4. Documentation Audit | Medical necessity language present; BCBA supervision documented; time blocks accurate | Clinical team/billing | Before claim release |
| 5. Claim Scrubbing | Duplicate check; time conflict check; NPI enrollment confirmed | Billing system + billing team | At submission |
| 6. Submission Quality Check | Clean claim confirmed via clearinghouse receipt | Billing team | Day of submission |
| 7. KPI Monitoring | Denial rate, FPRR, days in AR reviewed weekly | RCM manager | Weekly |
What Should ABA Practices Do After a Claim Is Denied?
Step 1: Categorize:
Divide denials into CARC codes and by Payer groups. All denials with the same CARC code should be batched together.
Step 2: Root Cause Analysis:
Is it coding, documentation, authorization, credentialing, or something else? Never rebill or reappeal until you address the issue.
Step 3: Appeal or Corrected Claim Decision:
- Coding or information error: Corrected claim (frequency code 7) with original ICN/TCN
- Medical necessity or authorization denial: Written appeal with updated clinical documentation
- Payer error: Reconsideration request with original submission evidence
Step 4: Follow-up Timeline:
- Day 10: First status check on submitted appeal or corrected claim
- Day 20: Second follow-up; escalate if no response
- Day 30: Escalate to peer-to-peer review for high-dollar medical necessity denials
Step 5: Revenue Tracking:
Track Revenue and patterns. Month-over-month denial trends can highlight and expose systemic issues that may not be otherwise obvious. Keep a file or use denial management software to record every denial, root cause, action, and result.
Which KPIs Should Every ABA Practice Monitor?
| KPI | Benchmark | Warning Threshold | Why It Matters |
|---|---|---|---|
| Clean Claim Rate | 95%+. | Below 90% | First-pass acceptance determines billing efficiency |
| First Pass Resolution Rate | 90%+ | Below 85% | Measures the quality of submission and coding |
| Denial Rate | Under 5% | Above 10% | ABA average runs 15 to 22% — significant improvement potential |
| Days in AR | Under 35 | Above 50 | Measures the speed of the full billing cycle |
| Net Collection Rate | 95%+ | Below 90% | Measures what is actually collected vs. what is owed |
| Authorization Approval Rate | 85%+ | Below 75% | Low rate signals documentation or payer relationship issues |
| Appeal Success Rate | 60%+ | Below 40% | Low-rate signal appeals are not well-documented |
How Can Technology Reduce ABA Billing Denials?
- Real-time patient eligibility verification: Automated clearinghouse transactions occur on every visit, identifying changes to coverage, errors in routing ABA carve-out codes, or payer switches before service delivery.
- Authorization tracking with AI alerts: Solutions that provide alerts on active authorizations, used session time, and expiration dates negate the calendar, which breaks down in scale.
- AI-assisted coding review: Claim scrubbing tools that flag CPT vs. H-code mismatches, missing modifiers, and time overlap conflicts before submission.
- Behavioral health RCM analytics: Denials can be identified and analyzed based on CARC code and by payer to identify systemic process issues that impact the bottom line.
- Behavioral health RPA automation: Automated tasks, such as submitting claims for clearinghouse processing and posting EOBs (ERAs), can be offloaded, eliminating manual labor.
Stop Losing Revenue You Have Already Earned.
BehavioralProz provides comprehensive ABA billing services, CPT coding, H-code billing, authorization management, credentialing, denial recovery, and behavioral health RCM analytics for autism practices at every stage of growth.
Frequently Asked Questions
Why are ABA claims denied?
Lack of valid prior authorization (expired or missing), incorrect H-Code or CPT-Code, absent modifiers, lapses in RBT credentialing, and poor documentation failing to support medical necessity.
What is the biggest reason ABA claims get rejected?
Missing or expired prior authorization is the leading cause of ABA claim denials, followed by incorrect payer code sets and credentialing gaps for new RBTs or BCBAs.
How can ABA providers reduce claim denials?
Automate real-time eligibility verification and authorization validity checks (alert 21 days prior), maintain and consult an up-to-date payer-specific code guide, and generate monthly denial trend reports segmented by CARC Code to implement systematic root cause corrections.
How long do ABA appeals take?
First-level ABA appeals usually get decided by payers in about 30-60 days. Requests for peer-to-peer reviews often get scheduled within 5-10 days of being placed, and requests for clarification on claims can be expected within similar timelines as initial appeals. The follow-up after the appeal is on the 10th and 20th days.
What is the difference between an ABA claim rejection and a denial?
A rejection fails technical edits before reaching the payer; it was never adjudicated. A denial entered the payer’s system and was refused with a documented reason code. Rejections are corrected and resubmitted; denials require an appeal or a corrected claim submission.
What CPT codes are used for ABA billing?
Top CPT-Codes 97151 (behavioral assessment), 97153 (tech-delivered services), 97155 (BCBA modifying protocol), 97156 (caregiver training), and 97158 (group treatment with BCBA on staff) are used for ABA. However, some Medicaid programs have preferred specific H Codes.
Can I bill 97153 and 97155 on the same day?
Yes, 97153 (RBT direct therapy) and 97155 (BCBA protocol modification) can be billed concurrently when the BCBA is present and actively modifying the protocol during the RBT’s session. Both require separate time documentation.
Why are ABA claims denied for untimely filing?
In many cases, the timely filing deadline runs 90 to 180 days after the date of service, depending on the payer. Any denials that fall to the wayside and remain unworked can quickly exceed these limits, rendering them unrecoverable no matter how accurate your coding or documentation may be.
How do I appeal a denial of medical necessity for ABA services?
Submit a written appeal with updated clinical documentation addressing the payer’s specific medical necessity criteria, including autism diagnosis, treatment plan goals, BCBA assessment, and progress notes reflecting measurable behavioral progress. Request a peer-to-peer review for high-dollar denials.