
Table of Contents
A majority of the behavioral health clinics have never renegotiated a payer contract. They sign up when their practices open with a payer and feel the rates seem acceptable for now. Years go by.
The rates never change.
The cost of providing the services rises. The rates don’t. This pattern is common and typical of how the majority of behavioral health providers around the country are working. Most simply don’t realize that by doing nothing, they are leaving 10 to 20% of their potential revenue on the table each year, not from billing and denials, but from not asking for more from their payers.
What Are Behavioral Health Payer Rates and Why Do They Matter?
Behavioral health payer rates are the amounts insurance companies will pay you to provide behavioral health services. These payments are listed as a code (CPT or HCPCS) within a payer’s contract, and these payments change from contract to contract.
These contract terms and their associated payments are negotiated prices that are impacted by a variety of factors, including the specific payer, region of the county, provider’s specialty, and either provider or payer’s clout in the contract negotiation.
Behavioral health payer rates represent the basis of the revenue your behavioral health practice collects. A $30 payment difference in reimbursement for the 90837 services that the practice bills 200 times each month from a particular payer represents $72,000 in lost revenue year over year for just one payer contract alone. Whether you choose to accept an initial proposed offer or push for more in the contract terms is far from just an administrative matter. It’s a financial one that carries exponentially impactful, long-term effects.
Your Payer Rates Are Older Than You Think.
Most behavioral health practices have not reviewed their fee schedules in 3 to 7 years. BehavioralProz conducts payer rate benchmarking and contract analysis to identify where your practice is leaving money on the table.
Why Are Behavioral Health Practices Often Paid Less Than They Should Be?
These are the patterns that keep practices stuck at submarket rates:
- Rates never reviewed: This is the most common, least sophisticated issue. A payer contract is signed, the clinician gets credentialed, and then the rate is just there on paper forever. No one revisits the payment structure at any point.
- No benchmarking data: Practices are unaware of what other providers in their service area with identical credentials and similar patient populations are receiving for the same codes. Without data comparing what peers earn, you can’t prove you are earning less.
- Negotiation avoidance: Many providers assume payer contracts are non-negotiable. They are not. Most payers expect contract renegotiation and have internal processes for it.
- No contract management system: Renewal dates pass unnoticed. The window to negotiate before auto-renewal closes without action.
- MHPAEA disparity accepted as normal: Many behavioral health providers receive lower reimbursement than medical/surgical providers for equivalent services. This is often a parity violation. Very few practices identify or challenge it.
A therapist posted in an AAPC community forum: “I just found out my Aetna rate for 90837 is $127. A colleague in the same zip code with the same license and credentials is getting $158 from the same payer. I signed in 2019 and never asked for a review.”
That $31 per session difference, at 150 sessions per month, is $55,800 per year from one payer.
Which Payers Should You Prioritize During Contract Negotiations?
| Payer Type | Negotiation Potential | Typical Challenges | Revenue Impact | Priority |
|---|---|---|---|---|
| Commercial Insurance (non-MBHO) | High | Requires data-backed request; internal process varies | High | First |
| MBHO Carve-Outs (Optum BH, Carelon, Magellan) | Moderate to High | Separate from base plan; ABA and SUD rates especially negotiable | High | First |
| Regional and Local Health Plans | High | Smaller plans have more flexibility; higher leverage for large practices | Moderate to High | Second |
| Medicare Advantage | Moderate | Rates often tied to Medicare fee schedule; limited but possible | Moderate | Second |
| Employer-Based Direct Contracts | High | Direct relationship; no intermediary; best rate potential | High (volume-dependent) | When volume justifies |
| Traditional Medicaid (fee-for-service) | Low | State-set rates; limited individual negotiation | Low | Unlikely |
| Medicaid Managed Care (MCOs) | Moderate | Some MCOs negotiate above state base rate; worth pursuing | Moderate | Third |
How Can You Prepare Before Negotiating With Insurance Companies?
Preparation is where negotiation is won or lost. Practices that enter a rate conversation with data negotiate from strength. Those that enter without it negotiate from hope.
Pre-negotiation preparation checklist:
- [ ] Pull your current fee schedule from every active payer contract
- [ ] Compare current rates to Medicare fee schedule for the same CPT codes in your geographic area (Medicare rate is a public benchmark reference)
- [ ] Request reimbursement data from industry benchmarking sources (MGMA, FAIR Health, state medical associations)
- [ ] Calculate your current net collection rate per payer; this identifies which payers are underperforming
- [ ] Review your denial rate per payer; low denial rates demonstrate clean billing performance (a negotiation asset)
- [ ] Document your patient volume per payer; large patient panels give you leverage
- [ ] Identify your specialty and any access-to-care gaps in your market (shortage areas, waitlists, underserved populations)
- [ ] Document any quality or outcome metrics your practice tracks
Which Data Points Give You More Leverage During Negotiations?
| Data Point | Why It Matters | How to Present It |
|---|---|---|
| Patient volume per payer | Large panels give leverage; removing your practice from the network would hurt the payer's adequacy | "We currently serve X patients enrolled in your plan" |
| Access-to-care metrics | Payers face network adequacy requirements; psychiatry and ABA have documented shortages | Reference your specialty's shortage data in your region |
| Appointment availability | Short wait times support network adequacy arguments | "New patient appointments available within 5 days" |
| Denial rate | Low rates demonstrate billing quality and reduce payer administrative burden | "Our clean claim rate is 96% above the behavioral health average" |
| Outcome data | Quality programs support medical necessity and value arguments | Patient improvement rates, discharge outcomes, completion rates |
| Geographic coverage | Rural or underserved areas with limited alternatives | Maps or data showing your service area relative to population need |
| Staff credentials | Board certifications, specialty training, additional service lines | Credentials list, specialized training documentation |
What Negotiation Mistakes Cost Behavioral Health Practices Thousands?
Why Do Practices Accept Initial Payer Offers?
Problem: A payer sends an enrollment packet with a fee schedule. The practice signs it without counter-proposing.
Revenue impact: Initial offers are almost always the payer’s floor, not their ceiling. Accepting without negotiation sets a rate baseline that may persist for years.
Solution: Never sign an initial fee schedule without a counter-proposal. Request the highest-performing fee schedule tier the payer offers for your specialty.
Why Is Benchmarking Often Ignored?
Problem: Practices do not know what comparable providers in their market earn for the same codes. Without that data, they have no basis for a negotiation request.
Revenue impact: Practices may be 10 to 30% below market without knowing it.
Solution: Use FAIR Health, MGMA survey data, CMS fee schedules, and state association resources to benchmark your rates annually.
Rate Negotiation Is One Revenue Lever. Here Are the Rest.
The Behavioral Health Operations Playbook covers payer contracting, denial prevention, AR recovery, RCM KPIs, and operational benchmarks built for practices ready to grow revenue systematically.
Why Do Providers Wait Too Long to Renegotiate?
Problem: Renegotiation conversations are deferred because they feel uncomfortable, complex, or low priority relative to clinical work.
Revenue impact: Each year at a submarket rate is a year of lost compounding revenue. A $25 rate increase negotiated in year 3 instead of year 1 represents $25 multiplied by session volume multiplied by two lost years.
Solution: Build contract review into your annual calendar. Set a reminder for 90 days before every payer contract renewal date.
Why Do Practices Focus Only On Fee Increases?
Problem: Rate negotiation often means asking for higher fees. That is only one lever.
Revenue impact: Other contract terms billing frequency, timely payment guarantees, audit provisions, dispute resolution terms affect cash flow and operational risk significantly.
Solution: Review the full contract, not just the fee schedule. Terms around claim submission deadlines, interest on delayed payments, audit recoupment limits, and network termination notice periods all affect your financial position.
RELATED READING


Why Do Practices Fail to Track Contract Performance?
Problem: A renegotiated rate is signed. No one tracks whether the payer is actually paying at the new rate.
Revenue impact: Systematic underpayment against the contracted rate goes undetected for months. For a $10 underpayment per session at 200 sessions per month, that is $24,000 per year in silent losses.
Solution: Build a contracted rate vs. paid rate reconciliation into your monthly AR review. Flag any payer where actual payments are running below contracted amounts.
Why Are Contract Renewal Dates Missed?
Problem: Payer contracts auto-renew if not renegotiated before the renewal date. The window to negotiate opens and closes without anyone acting on it.
Solution: Track every contract renewal date in a central system with alerts at 120 days and 60 days before renewal.
How Much Additional Revenue Can Better Payer Rates Generate?
Scenario: A 5% rate increase across all commercial payers
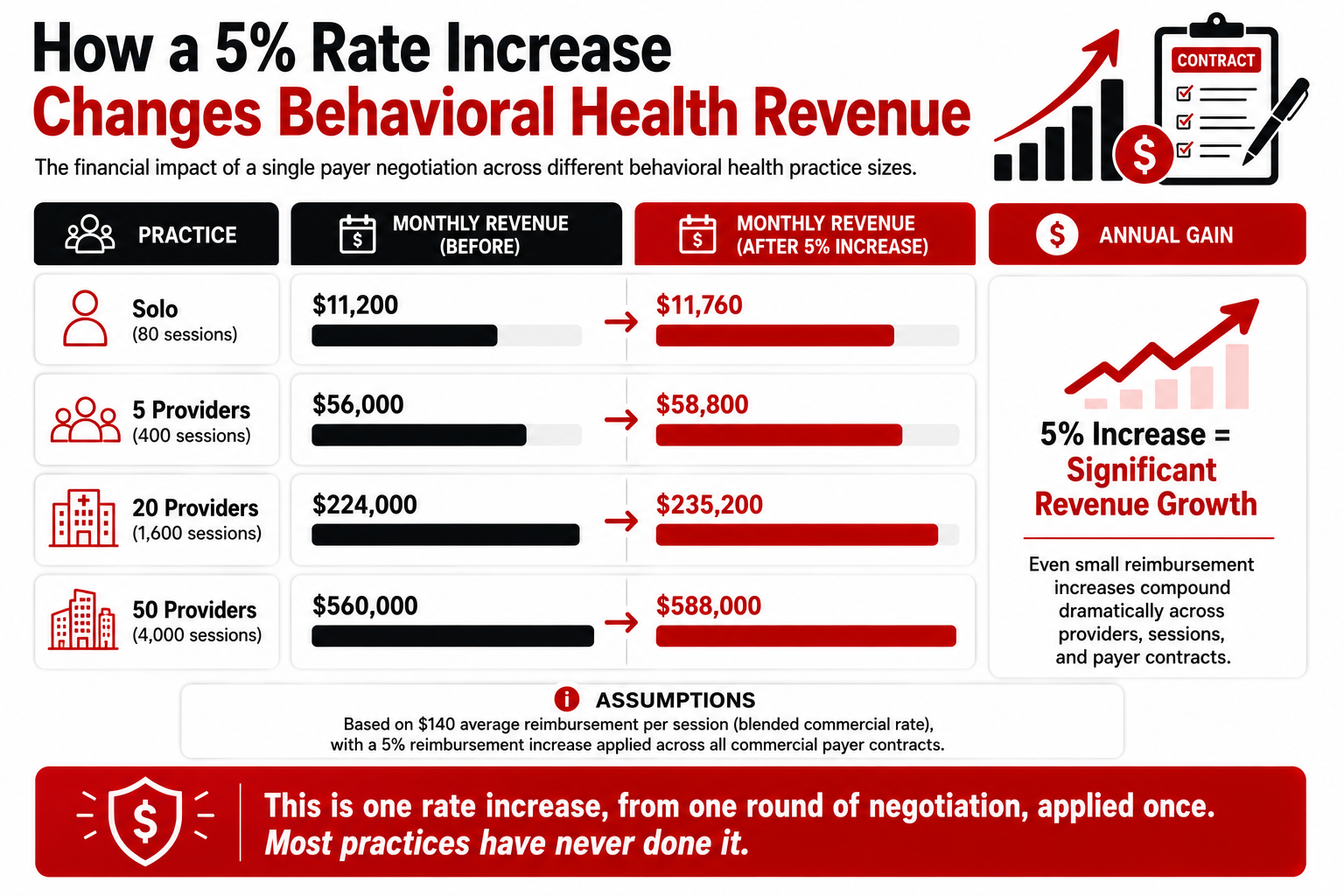
These numbers assume only a 5% increase on commercial payers. Practices that have never renegotiated often find 10 to 20% gaps relative to market rates. The upside is proportionally larger.
When Should You Renegotiate Existing Payer Contracts?
- Contract Anniversary: Many payer contracts will allow renegotiation within 60-90 days of the annual renewal date.
- Practice Growth: When adding additional providers, your patient volume directly expands, an immediate leverage argument to present to a payer.
- New Service Lines: When adding a new program, like an IOP, PHP, telehealth, or ABA program, this may warrant a contract renegotiation.
- Market Changes: When there is a recognized shortage of providers in your specialty and geographic area, this supports an access-to-care argument.
- Payer Underperformance: When a specific payer begins experiencing increased denial rates or has a track record of underpaying your services, this provides a clear argument to discuss contract performance.
Should Behavioral Health Practices Outsource Payer Negotiations?
Outsourcing is worth evaluating when:
- The practice lacks internal expertise on payer contract language and benchmarking data
- The volume of contracts makes internal management impractical (10+ payer contracts)
- Prior self-negotiation attempts have not produced results
- The practice is adding locations or providers at a pace that creates new contracting needs regularly
The ROI case: A negotiation that produces a 5% rate increase for a 20-provider practice generates $134,400 annually. A contracting consultant who charges $5,000 to $15,000 for that project delivers a 9x to 27x return.
Be cautious of: Firms that charge ongoing percentages of rate increases negotiated (conflicts of interest), or that cannot provide specific behavioral health contracting experience.
7 Step-By-Step Process for Successful Contract Negotiations
| Step | Action | Timeline |
|---|---|---|
| 1. Data Collection | Pull current rates, session volumes, denial rates, net collection rates per payer | Week 1 |
| 2. Benchmarking | Compare current rates against Medicare, FAIR Health, and regional data | Week 1 to 2 |
| 3. Proposal Creation | Prepare a written rate proposal with supporting data and access-to-care context | Week 2 |
| 4. Negotiation Initiation | Contact payer's provider relations or contracting department in writing | Week 3 |
| 5. Negotiation Meeting | Present data; respond to payer counteroffers with documented rationale | Week 4 to 6 |
| 6. Contract Review | Review proposed terms beyond fee schedule; negotiate non-rate provisions | Week 6 to 8 |
| 7. Performance Monitoring | After new rates take effect, reconcile actual payments against contracted rates monthly | Ongoing |
Stop Accepting What Payers First Offer.
BehavioralProz provides behavioral health contracting support, rate benchmarking, and revenue optimization for practices that are ready to close the gap between current rates and what the market supports.
Frequently Asked Questions
How often should behavioral health practices renegotiate payer contracts?
Ideally, every year at renewal. After major growth like adding providers, opening new sites, or broadening services (all of which give you negotiating power), do so again.
Can therapists negotiate insurance reimbursement rates?
Yes. Any of your payer contracts can be renegotiated. The process for requesting new rate schedules from each provider varies but, in most cases, exists. Use data to back up any rate requests (especially for practices serving larger patient populations or specialties that are underserved) and increase your likelihood of success.
What is a good reimbursement rate for mental health services?
Reimbursement rates vary by region, specialty, and payer. As a benchmark, compare your rates to the Medicare fee schedule for your ZIP code (public reference) and FAIR Health regional data. Practices receiving less than 90% of the Medicare fee schedule for behavioral health codes typically have negotiation upside.
Can a billing company help negotiate payer contracts?
If you are currently working with a behavioral health RCM provider, inquire if they include contracted negotiations as part of their suite of services. If you don’t have internal contracting expertise, an RCM’s negotiations services (with outdated contracts) can bring a good ROI.
Do ABA providers negotiate payer rates?
Yes, ABA providers have their own contracting processes separate from other behavioral health providers within the health plan and can negotiate with payers for those rates. While H-code rates like H2014 or H2019 are usually set on the initial contract, they are negotiable with their dedicated ABA contracting department.
How do commercial payer contracts differ from Medicaid contracts?
While commercial payer contracts are individually negotiable, the majority of state-run Medicaid fee schedules remain set. Your client might be a member of a managed care organization which, in some cases, negotiates at a higher than state rate with its providers.