
Table of Contents
A new PMHNP joins a group practice. She submits credentials the day she starts. 8 weeks in, she’s seen 150 patients, but their sessions are not able to be billed in-network as the payer’s effective enrollment date has not been issued. The group practices are either writing off the revenue, trying (seldom successfully) to get in-network retroactively, or are billing out-of-network at a very low percentage of contracted rates.
This is not an exception; this is the normal if credentialing is being managed as if it were a start date deliverable rather than a lead time project.
Behavioral health practices lose far more revenue to credentialing errors than owners suspect not to one spectacular fail, but rather a death by a thousand cuts of missed payer connections, backdating failures, and missed and failed renewal applications.
What Is Behavioral Health Credentialing?
Behavioral health credentialing involves insurers validating your background, training, and practice information before they’ll add you to their provider network. Your ability to bill their plans in-network only starts once this complex process concludes. Until it does, you either can’t bill their plans at all, or you have to bill at very unfavorable out-of-network reimbursement rates.
Credentialing is not a single application. It is a series of payer-specific enrollment processes, each with its own documentation requirements, timelines, and approval workflows. Behavioral health adds complexity: MBHO carve-outs require separate enrollment from the base commercial plan, and specialty designations (BCBA, PMHNP, LCSW) trigger payer-specific eligibility rules that generalist enrollment processes frequently miss.
Credentialing Delays Are Costing Your Practice Every Day You Wait.
BehavioralProz manages behavioral health credentialing from application through approval, including MBHO carve-out enrollment, CAQH maintenance, recredentialing, and multi-state payer enrollment.
Why Do Credentialing Mistakes Cost Practices Thousands?
The cost of a credentialing delay is not abstract. It is the number of sessions delivered multiplied by the difference between in-network and out-of-network reimbursement, for every day the enrollment is pending.
| Enrollment Delay | Sessions/Week | In-Network Rate | Revenue at Risk |
|---|---|---|---|
| 30 days | 20 | $150 | $12,000 |
| 60 days | 20 | $150 | $24,000 |
| 90 days | 20 | $150 | $36,000 |
| 120 days | 20 | $150 | $48,000 |
For a busy provider, a 90-day delay is not a minor inconvenience. It is a $36,000 problem that could have been prevented by submitting the application 90 days before the first scheduled session.
7 Most Common Behavioral Health Credentialing Mistakes
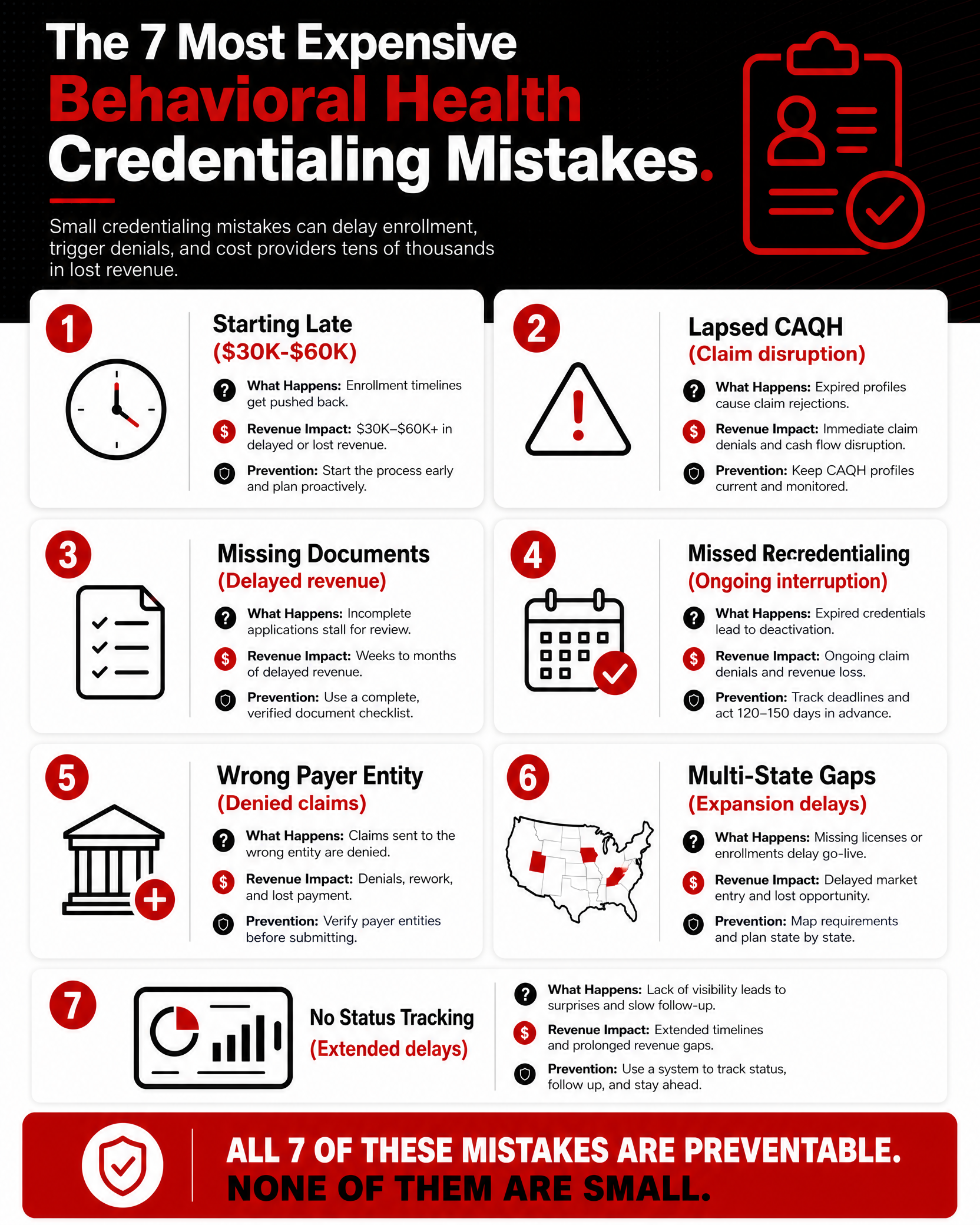
Credentialing mistakes cost behavioral health practices thousands in delayed reimbursements and lost contracts. Here are the seven mistakes that derail providers most often:
- Starting Credentialing Too Late Costs Behavioral Health Practices Thousands
- An Outdated CAQH Profile Is a Silent Revenue Killer
- Incomplete Applications Are the Leading Cause of Credentialing Rejections
- Missing Recredentialing Deadlines Can Terminate Payer Contracts
- Credentialing to the Wrong Payer Entity Voids Your Application
- Multi-State Providers Face Separate Enrollment Requirements in Every State
- Untracked Applications Lead to Months of Lost Reimbursements
#1 Why Do Providers Wait Too Long to Start Credentialing?
What happens: The provider is hired, credentialing starts on the start date, and the practice discovers the payer takes 90 to 120 days to process enrollment. The first 90 days of the provider’s sessions are either unbillable in-network or billed out-of-network.
Why it occurs: Credentialing feels like an administrative task that belongs to the onboarding checklist, not a financial project that should start at the offer letter.
Revenue impact: $30,000 to $60,000 per provider, depending on volume and payer mix.
How to avoid it: Begin credentialing applications the day a provider signs their offer letter. Target a 90-day lead time minimum for commercial payers; 120 days for MBHO carve-outs and Medicaid.
#2 Why Is an Outdated CAQH Profile a Major Problem?
What happens: CAQH ProView requires re-attestation every 120 days. When the deadline passes without re-attestation, the provider’s profile becomes inactive. Payers that use CAQH for credentialing data automatically suspend enrollment, generating denials across every affected payer simultaneously.
Why it occurs: No one owns the CAQH re-attestation calendar. The 120-day deadline passes unnoticed.
Revenue impact: Every payer using CAQH for this provider stops paying until re-attestation is completed and the payer’s enrollment is reactivated a process that takes 2 to 4 weeks per payer.
How to avoid it: Set calendar alerts at 90 days, 30 days, and 7 days before CAQH attestation expiration for every active provider. Assign one owner across the organization.
#3 Why Do Applications Get Rejected for Missing or Incorrect Documents?
What happens: An enrollment application is submitted with an expired malpractice certificate, a license copy missing the renewal date, or a CV with unexplained gaps. The payer returns the application and the credentialing clock restarts.
Why it occurs: Applications are assembled quickly without a pre-submission document audit.
Common document errors:
- Malpractice certificate expired before approval is issued
- License copy does not show expiration date clearly
- CV gaps over 30 days without written explanation
- Board certification copy missing the certificate number
- NPI taxonomy code mismatch between application and claim
How to avoid it: Use a pre-submission document checklist. Verify every document against its expiration date before the application goes out.
Credentialing Is Just One Piece. Here's the Full Operational Picture.
The Behavioral Health Operations Playbook covers credentialing workflows, billing best practices, RCM KPIs, and denial prevention , everything a behavioral health practice needs to run efficiently from day one.
#4 Why Do Practices Ignore Recredentialing Deadlines?
What happens: Most payers require recredentialing every 2 to 3 years. Missed deadlines result in enrollment suspension; the provider is effectively removed from the payer’s network until recredentialing is completed.
Why it occurs: Recredentialing deadlines are tracked inconsistently or not at all. The deadline is discovered when a claim is denied.
Revenue impact: Every claim submitted to the suspended payer is denied until re-enrollment is approved, a process that takes 45 to 90 days.
How to avoid it: Maintain a credentialing calendar with recredentialing deadlines for every active payer-provider combination. Initiate recredentialing 90 days before the expiration date.
#5 Why Is Credentialing With the Wrong Payer Entities Costly?
What happens: A practice credentials with Aetna but not with Evernorth (Aetna’s behavioral health MBHO). Claims go to Aetna. The behavioral health benefit is managed by Evernorth. CO-B7 denials on every claim until the MBHO enrollment is completed.
Why it occurs: Staff credential with the commercial plan’s primary payer without investigating whether behavioral health benefits are carved out to a separate MBHO.
Revenue impact: Every claim for every patient with that payer is denied until MBHO enrollment is complete.
How to avoid it: Before submitting any commercial enrollment, confirm whether behavioral health is carved out. If it is, credential with both the base plan AND the MBHO as parallel applications, not sequential ones.
#6 Why Do Multi-State Providers Run Into Enrollment Issues?
What happens: A practice expands to a second state. The providers are licensed in both states. But they are only credentialed with Medicaid in one state, and each state’s Medicaid program and managed care organizations require independent enrollment.
Why it occurs: Commercial credentialing transfers conceptually across state lines. Medicaid enrollment does not. Each state Medicaid program is independent.
Revenue impact: An entire location may be unbillable for Medicaid until state-specific enrollment is complete. For community mental health and SUD programs serving Medicaid patients primarily, this is a significant operational crisis.
How to avoid it: When entering a new state market, build a state-specific enrollment checklist that covers state Medicaid, the state’s managed care organizations (MCOs), and state-specific MBHO contracts. Start this process 120 to 180 days before the location opens.
#7 Why Do Providers Fail to Track Application Status?
What happens: An application is submitted. No one follows up. The payer returns an information request. It goes unread for 30 days. The credentialing timeline extends by 30 to 60 days because of a document the payer needed, and nobody knew they asked for.
Why it occurs: Credentialing is treated as a submission task, not an ongoing monitoring responsibility.
How to avoid it: Follow up with every payer at day 30, day 60, and day 90 after submission. Ask specifically: Is this application complete? Is anything outstanding? Get a representative name and reference number on every call.
RELATED READING


What Credentialing Documents Should Every Behavioral Health Provider Maintain?
| Document | Notes | Renewal Frequency |
|---|---|---|
| CAQH ProView Profile | Re-attest every 120 days; must be authorized for target payers | Every 120 days |
| State License(s) | Current copy; expiration date visible; license in every practice state | Per state renewal cycle |
| DEA Certificate | Required for prescribers; current; same state as practice | Every 3 years |
| NPI (Type 1 and 2) | Individual + group NPI; taxonomy codes confirmed | No expiration; update if scope changes |
| Board Certification | If applicable; current certificate with number | Per board renewal cycle |
| Malpractice Insurance | Certificate naming practice; $1M/$3M or payer-required limits; retroactive dates | Annual |
| CV / Work History | No unexplained gaps; covers last 10 years | Update with each new position |
| W-9 | Practice taxpayer ID; current | When EIN changes |
| Residency / Training | Completion letters; required for psychiatrists and other medical providers | Once (at initial credentialing) |
| Collaborative Agreement | Required in some states for PMHNPs | Per state requirements |
How Long Does Behavioral Health Credentialing Actually Take?
| Payer / Program | Typical Timeline | Key Variables |
|---|---|---|
| Medicare (PECOS) | 60 to 90 days | Complete application; no gaps |
| Medicaid (state-specific) | 90 to 180 days | State varies significantly |
| Commercial (Aetna, Cigna, BCBS) | 60 to 90 days | CAQH profile complete; no missing docs |
| MBHO Carve-Outs (Optum BH, Carelon, Magellan) | 90 to 120 days | Separate from base plan; often longer |
| ABA-specific payer credentialing | 90 to 150 days | ABA departments have separate workflows |
| Telehealth-only platforms | 30 to 60 days | Some platforms have expedited enrollment |
These timelines assume complete, error-free applications submitted with all required documentation. Missing documents, CAQH lapse, or application errors add 30 to 60 days per occurrence.
What Credentialing Challenges Are Unique to Behavioral Health Providers?
PMHNPs: Many commercial payors and MBHOs do not credential PMHNPs alone and require that a supervising physician collaboration agreement is on file. Even if this isn’t a requirement in the state, it is at the payor level, so verify PMHNP credentialing requirements for specific payors before applying.
ABA providers: At many commercial payors and MBHOs, ABA enrollment runs through separate departments. You’ll need BCBA verification through BACB and sometimes supervised hours documentation. Begin ABA enrollment sooner rather than later.
Telehealth credentialing: A therapist providing telehealth to clients across multiple states needs to be licensed in each client’s state of service at the time of the encounter. This is primarily a licensing issue that needs to be taken into account alongside your payor enrollments that span multiple states (multi-state licensing, interstate compacts, etc.).
SUD facilities: Outpatient SUD programs pursuing Medicaid enrollment generally need state behavioral health agency or SAMHSA certification prior to payor enrollment. Account for state and facility certification time in your project plan.
How Can Practices Build a Credentialing Process That Scales?
- Centralized tracking: One system (spreadsheet or credentialing software) tracking every provider, every payer, submission date, application status, approval date, effective date, and recredentialing deadline
- CAQH management calendar: 120-day re-attestation schedule for every active provider; automated alerts at 90, 30, and 7 days
- Document maintenance: Central document repository with expiration date tracking for licenses, malpractice certificates, DEA, and board certifications
- New hire protocol: Credentialing applications initiated at offer letter signing, minimum 90-day lead time built into hiring timelines
- Follow-up cadence: Payer contact at day 30, 60, and 90 post-submission; documented call records with representative name and reference number
- Recredentialing calendar: 90-day advance notice alerts for all payer recredentialing windows across every active provider
What Should Practices Do If Credentialing Is Delaying Revenue?
- Bill as out-of-network: Continue to collect during a delay in enrollment; reveal OON to patients prior to service.
- Attempt retroactive enrollment: Some payers allow retroactive effective dates on a case-by-case basis; ask at submission and document the request.
- Escalate to provider relations: These teams can often quicken enrollment if providers already have a completed application. Ask who the contact person is and what the process is to escalate the issue on your first call.
- Supervising provider billing: In some circumstances and within legal scope, a credentialed supervising provider can bill for services while the new provider’s enrollment is pending; confirm state and payer rules before attempting.
- Prioritize highest-volume payers first: When you are applying for multiple payers at once, handle the applications in order of your volume by payer.
Wrong Document. Wrong License Type. One Mistake Delays Everything.
Credentialing errors don’t announce themselves , they show up as delayed approvals and unbilled sessions 90 days later. BehavioralProz ensures every application is complete, correct, and actively followed up on.
Frequently Asked Questions
How long does behavioral health credentialing take?
60-90 days for commercial payers, 90-120 days for MBHO carve-outs (Optum, Carelon, Magellan), and 90-180 days for state Medicaid programs, depending on the state.
What is CAQH credentialing?
CAQH ProView is the provider database used by most commercial payers to verify your credentials. You’ll need to complete your profile and attest to its contents every 120 days. Failure to do so will put all providers using CAQH into suspension, effectively blocking any claims submission.
Can I bill before credentialing is complete?
Yes, you can bill out-of-network, but you can’t bill out as in-network until you have an effective enrollment date. Billing as in-network before the effective date will lead to retroactive denials. You can bill under a supervising provider during your credentialing process, but make sure this is allowed per payer and state.
What happens if my CAQH profile expires?
When your CAQH profile is not updated, payers with a feed from CAQH are notified. The notification may prompt the payer to suspend the provider’s enrollment. Any claims that are filed will be denied when in suspension. After re-attestation and notification, it typically takes 2-4 weeks per payer for reinstating the provider back to the plan.
How often do behavioral health providers need recredentialing?
The credentialing process is renewed on average every 2-3 years, depending on the payer’s requirements. When the credentialing cycle is missed, the provider will have their enrollment suspended until the re-credentialing is completed.
Which insurance companies should therapists credential with first?
You’ll want to target the payers that will cover the majority of your patient population. For typical outpatient providers, this means your local BCBS plan, Aetna/Evernorth, Cigna/Evernorth, United/Optum BH, and your state Medicaid. Simultaneously submit these, not sequentially.