Table of Contents
You didn’t get into mental health to manage billing. But here you are staring at a denial queue, trying to figure out why Optum keeps rejecting your 90837s, and wondering if your front desk person (who is also handling scheduling, phones, and intake) is actually submitting clean claims.
Or maybe you tried outsourcing once. The company seemed good on the call, promised clean submissions and fast turnaround, and then spent the next six months billing your group therapy sessions wrong and ignoring your emails.
So now you’re stuck between two options that both feel broken.
Here’s the thing: this is one of the most important operational decisions a mental health practice can make, and it’s almost always made with incomplete information. This guide is going to change that. We’ll look at real costs, real risks, and the factors that actually determine which model is right for your practice, not practices in general.
First, Let's Be Honest About What's Really Going On
The In-House Billing Trap Most Practices Don't See Coming
Most small and mid-sized mental health practices end up doing billing in-house by default, not by choice. A therapist starts taking insurance, handles billing themselves, then hires a front desk person who gradually absorbs billing responsibilities as the practice grows. Before long, billing is a fragile, informal process owned by one person who also does six other things.
“My biller just put in her notice, and I realized I have no idea what she was actually doing. I’m terrified of what I’m going to find.”
“We had a staff member managing billing for 4 years. When she left,t we discovered she hadn’t been submitting secondary claims for over a year. I’m still trying to recover that money.”
This isn’t a staffing failure. It’s a structural one. Behavioral health billing is genuinely complex work — more complex than most general practice billing — and building internal capacity to do it well requires systems, redundancy, and ongoing training that most practices simply don’t have.
Why "We Tried Outsourcing Once, And It Was A Disaster" Is More Common Than It Should Be?
The outsourcing horror stories are also real. Practices hire a billing company that turns out to be a generalist shop with no understanding of behavioral health payer rules, carve-outs, or the specific CPT codes that govern mental health services. Claims go out wrong. Denials pile up. The practice loses revenue and months of time trying to clean up the mess.
The lesson most people take from this is “outsourcing doesn’t work.” The actual lesson is: outsourcing to the wrong partner doesn’t work. A general medical billing company billing your 90837s and 90847s is like hiring an accountant who’s never filed a Schedule C to do your taxes. The gap between what they know and what you need is enormous.
Think Your Billing Is Fine?
Most Practices Are Wrong. Get a free billing audit and find out exactly what your practice is (and isn’t) collecting.
What Does In-House Mental Health Billing Actually Cost?
The Visible Costs
The obvious in-house billing costs are:
- Biller salary: $35,000–$55,000/year for a dedicated billing specialist (varies by region and experience)
- Benefits: Add 20–30% on top of salary for health insurance, payroll taxes, PTO
- Practice management/billing software: $200–$600/month depending on the platform (Kareo, SimplePractice, TherapyNotes, AdvancedMD)
- Clearinghouse fees: $50–$200/month
- Training and certifications: $500–$2,000/year
Ballpark visible cost: $55,000–$80,000/year for a dedicated biller with software and overhead.
For practices with no dedicated biller where the therapist or office manager handles billing, the cost is hidden in time, opportunity cost, and burnout.
The Hidden Costs (This Is Where Practices Really Lose Money)
The numbers above are just the floor. The real cost of in-house billing lives in the places you’re not tracking:
Denial rates and write-offs. The national average clean claim rate across medical specialties is around 95–97%. Most in-house behavioral health billing operations run 80–88%. That gap, 8 to 17% of claims hitting the denial queue, represents money that requires rework to recover. Rework takes time. Some of it never gets recovered at all. For a practice billing $500K/year, a 10% avoidable write-off rate is $50,000 in lost revenue.
Timely filing limits. Most payers require claims to be filed within 90–180 days of the date of service. When billing falls behind, which happens any time a biller is out sick, gives notice, or gets overwhelmed, claims fall outside the timely filing window and become uncollectable. This is a pure, 100% preventable revenue loss that happens constantly in under-resourced in-house operations.
Credentialing gaps and enrollment delays. In-house billers often manage credentialing alongside everything else. Credentialing a new clinician with a behavioral health carve-out payer like Optum Behavioral Health or Carelon Behavioral Health takes 60–120 days under normal conditions, longer if something goes wrong. Every day a credentialed therapist can’t bill in-network is lost revenue. Most practices don’t track this number. It’s usually significant.
Staff turnover. Billing staff at small practices have high turnover rates. Every time a biller leaves, there’s a 4–12 week gap to hire and train a replacement, and a 3–6 month ramp-up period before they’re fully competent. During that window, claims are delayed, denials go unworked, and errors increase.
Compliance exposure. Billing errors in mental health, particularly upcoding, modifier misuse, or documentation mismatches, can trigger payer audits or OIG scrutiny. In-house billers who haven’t had behavioral health-specific compliance training are a liability most practices don’t realize they’re carrying.
Real Cost-Per-Claim Breakdown
For an in-house operation processing 400–600 claims/month (typical for a mid-sized group practice):
| Cost Category | Monthly | Annual |
|---|---|---|
| Biller salary (prorated) | $3,800–$4,800 | $45,000–$58,000 |
| Benefits (25% of salary) | $950–$1,200 | $11,400–$14,400 |
| Software + clearinghouse | $400–$800 | $4,800–$9,600 |
| Estimated denial write-off (10%) | $4,000–$8,000 | $48,000–$96,000 |
| Total estimated cost | $9,150–$14,800 | $109,200–$178,000 |
At 500 claims/month, that’s roughly $18–$30 per claim fully loaded, and that’s assuming your biller is competent, fully trained, and not about to give their two weeks’ notice.
What Does Outsourced Mental Health Billing Actually Cost?
How Billing Companies Charge?
Most outsourced billing companies use one of two models:
Percentage of collections: The most common model. The billing company earns a percentage of what they actually collect, typically 5–10% for behavioral health. The range varies based on specialty complexity, volume, and payer mix. This model aligns incentives: they get paid more when you get paid more.
Flat fee per claim: Less common, but some companies charge a flat fee per submitted claim regardless of whether it’s paid. Be cautious of this model; it creates no incentive to follow up on denials or unpaid claims.
What You Should And Shouldn't Be Paying?
For behavioral health billing specifically:
- 5–7% of collections: Reasonable for a solo or small practice with a straightforward payer mix
- 7–10%: Expected for complex behavioral health (ABA, PHP/IOP, SUD, carve-out-heavy payer mix)
- Below 5%: Red flag likely a generalist company that will underperform on behavioral health
- Above 12%: Red flag on the other end unless you have extremely complex, high-value claims
A well-run outsourced billing relationship for a practice collecting $600K/year at 7% is $42,000/year, typically less than the fully loaded cost of one full-time in-house biller, and without the turnover risk, compliance exposure, or denial backlog.
The Difference Between A Generalist Biller And A Behavioral Health Specialist
This distinction cannot be overstated. Behavioral health billing has specific requirements that most general billers haven’t been trained on:
- Time-based CPT codes (90832, 90834, 90837, 90846, 90847, 90853) require documentation of start/stop times or total face-to-face time, a requirement many generalist billers miss
- Place of service codes, telehealth vs. office vs. outpatient hospital, carry different reimbursement rates and modifier requirements.
- MBHO carve-outs many commercial payers carve behavioral health to Optum Behavioral Health, Carelon Behavioral Health, or Magellan, requiring separate credentialing and different claims routing
- Mental Health Parity rules understanding when a denial may be a parity violation (and therefore legally challengeable) requires regulatory knowledge that most generalist billers don’t have.
- Prior authorization management for behavioral health has disproportionately high prior auth requirements; mismanaging these leads directly to retroactive denials.
Hire a generalist billing company for mental health services,s and you’ll spend more time managing them than you saved by outsourcing.
Side-by-Side Comparison: In-House vs. Outsourced Mental Health Billing
| Factor | In-House | Outsourced (Specialist) |
|---|---|---|
| Upfront control | High — you see everything | Varies — good partners offer full transparency |
| Real-time access | Immediate | Depends on platform access + reporting |
| Denial management | Depends entirely on staff quality | Typically stronger — it's their core function |
| Credentialing | Often ad hoc, error-prone | Usually systematized |
| Compliance | Only as good as your biller's training | Should be built into the process |
| Scalability | Requires hiring as you grow | Scales with your volume automatically |
| Turnover impact | High — you absorb all disruption | Minimal — vendor absorbs internally |
| BH-specific expertise | Rare unless you were hired for it | High with a specialist firm |
| True annual cost | $55K–$175K (fully loaded) | $25K–$60K (at 6–9% of collections) |
| Time investment from you | High (managing staff + billing oversight) | Low (once a good partner is in place) |
Multi-State Billing Is Complex. Your Operations Playbook Shouldn't Be.
The Behavioral Health Operations Playbook covers billing workflows, denial prevention, multi-state RCM strategy, and KPI benchmarks, everything a behavioral health organization needs to operate efficiently across states.
When In-House Billing Makes Sense (And When It Doesn't)?
In-house billing is actually the right answer in a few specific situations:
You have high volume and a dedicated billing staff. If your practice bills $2M+/year and you have two or more dedicated billing employees (not staff who also do other things), the economics can work in-house, provided you’ve invested in training, software, and compliance protocols.
You have a billing manager with behavioral health-specific training. A CPC (Certified Professional Coder) or CBCS (Certified Billing and Coding Specialist) who has worked specifically in behavioral health is a real asset. If you have this person and they’re not going anywhere, in-house makes sense.
You need extreme payer-specific customization. Some complex multisite facilities with negotiated contracts and highly custom billing workflows are genuinely better served by building an internal revenue cycle department.
It does NOT make sense when:
- One person handles billing AND everything else
- You don’t know your clean claim rate, denial rate, or average days in AR
- Your biller has never received behavioral health-specific training
- You’ve had significant staff turnover in the billing role in the last 2 years
- You’re adding clinicians, and billing volume is outpacing your staff’s capacity
When Outsourcing Makes Sense (And What to Look For?)
Outsourcing is the right move for the majority of mental health practices, but only with the right partner. Here’s when to make the move:
- You’re a solo or group practice billing between $150K–$2M/year
- You’re opening a new practice and can’t afford to build a billing infrastructure from scratch
- You’ve just had billing staff leave, and you’re staring at a denial backlog
- You’re adding clinicians,s and the billing load is outpacing your internal capacity
- You want to offer more insurance options, but don’t have the credentialing bandwidth
What to look for in an outsourced behavioral health billing partner:
- Behavioral health-specific experience: Ask which mental health CPT codes they bill most, how they handle carve-out payers, and what their denial rate is. If they can’t answer these questions specifically, walk away.
- Transparent reporting: You should have access to a live dashboard showing your AR, claim status, denial trends, and collection rates. If they’re not offering this, it’s a red flag.
- Clear denial management process. What happens when a claim is denied? Who follows up, how quickly, and what’s the escalation process for parity-based denials?
- Credentialing capabilities: Behavioral health credentialing is its own specialty. Not every billing company handles it well.
- A dedicated point of contact: A specific person or team who knows your practice.
HIPAA-compliant infrastructure, BAA (Business Associate Agreement) in place before any data is shared.
The 5 Mistakes Practices Make When Making This Decision
Making The Decision Based On Fear Of Losing Control
Control is important. But “control” of a broken process is not actually control; it’s just proximity to the problem. A good outsourcing partner gives you better visibility into your revenue cycle than most in-house operations provide.
Choosing An Outsourced Partner On Price Alone
A billing company charging 4% of collections sounds better than one charging 8% until you realize the 4% company’s denial rate is 25% and they’re writing off everything over 90 days. In behavioral health billing, you get what you pay for.
Assuming The Current Person "Has It Handled."
This is the most dangerous assumption in medical billing. A practice that doesn’t audit its billing at least annually has no idea what it’s actually losing. Denial patterns, write-off rates, unapplied credits, and timely filing misses can quietly drain revenue for months before anyone notices.
Not Accounting For Credentialing When Evaluating The Decision
Credentialing is not billing. But they’re deeply connected; billing errors often trace back to credentialing errors (wrong NPI on file, inactive enrollment, specialty mismatch). If you’re evaluating billing options without also evaluating credentialing support, you’re solving half the problem.
Treating This As A Permanent, Irreversible Decision
You can change billing models. You can transition to outsourced billing, find out the partner isn’t right for you, and course-correct. The goal isn’t to find the perfect theoretical model; it’s to find the right fit for where your practice is right now, one that can evolve.
A Note on Behavioral Health–Specific Billing Complexity
This is worth stating plainly, because it’s often understated: mental health and behavioral health billing is harder than most other specialties.
This isn’t because the codes are more complicated (though they are). It’s because of the payer environment:
- Behavioral health is disproportionately carved out to managed behavioral health organizations (MBHOs), such as Optum Behavioral Health, Carelon (formerly Beacon), Magellan, and others, each with its own credentialing processes, prior auth requirements, and billing rules.
- The Mental Health Parity and Addiction Equity Act (MHPAEA) creates legal protections for behavioral health beneficiaries, but enforcing those protections requires someone who knows they exist and knows how to document violations.
- Prior authorization requirements for behavioral health services are applied at higher rates than comparable medical/surgical services, a documented disparity that is itself a parity violation in many cases.
- Telehealth billing rules for behavioral health services vary by state, payer, and platform, and they’ve been in flux since 2020.
If you’re evaluating billing solutions in-house or outsourced and the person you’re talking to doesn’t know what a behavioral health carve-out is, doesn’t know the difference between 90837 and 90847, and can’t explain what MHPAEA means for your denial appeals, they are not the right person to manage your revenue cycle.
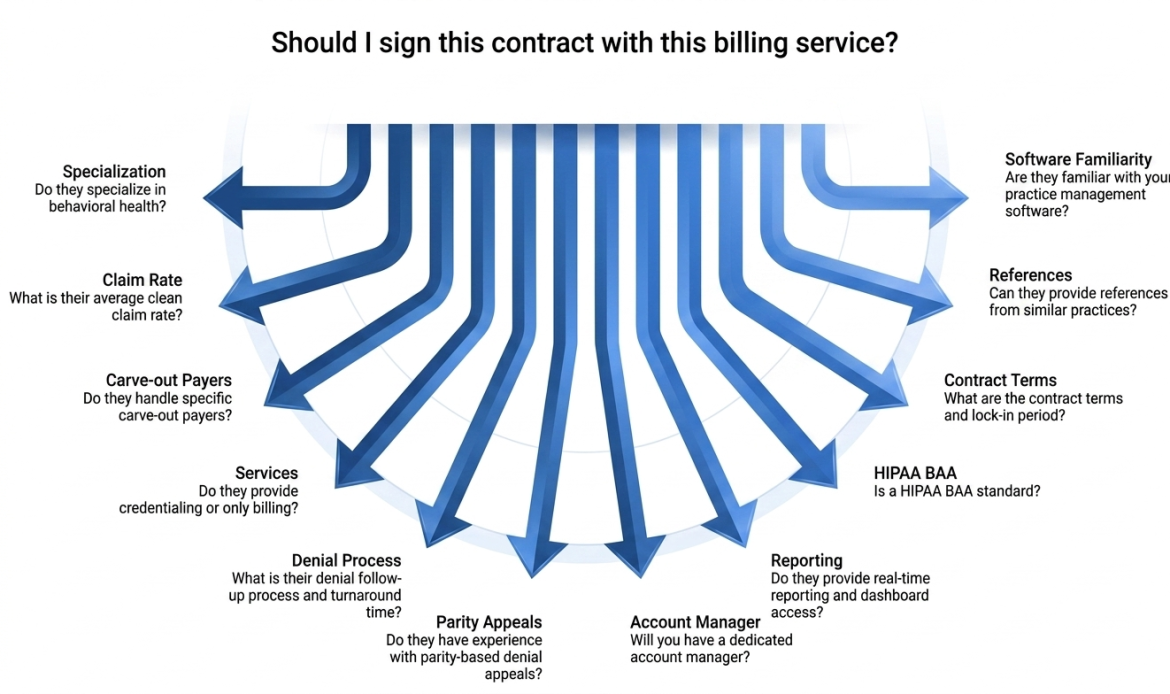
How to Evaluate an Outsourced Billing Partner — Checklist?
Run through this checklist every time you’re close to finalizing an agreement, so you clearly understand the partner’s services, pricing, compliance, and other terms before committing your practice’s revenue cycle to them.
Have Questions About Your Specific Billing Situation?
Schedule a 20‑minute call with our billing team and we’ll take a close look at your current setup, workflows, and performance.
Frequently Asked Questions
Is it cheaper to bill insurance in-house or outsource mental health billing?
In most cases, outsourcing mental health billing is less expensive than maintaining a fully-staffed in-house billing operation once all costs are accounted for. An in-house biller for a mental health practice costs $55,000–$80,000+ per year in salary, benefits, and software. Outsourced behavioral health billing typically runs 6–9% of collections, which, for a practice collecting $600K/year, is $36,000–$54,000/year, often with better denial management and no turnover risk.
What percentage do outsourced mental health billing companies charge?
Outsourced mental health billing companies typically charge between 5–10% of collected revenue. For behavioral health specifically, 6–8% is the typical market range for a specialist firm. Rates below 5% often signal a generalist company that may underperform on behavioral health–specific payer rules. Rates above 12% are generally not justified unless the practice has unusually complex billing needs.
What are the risks of outsourcing mental health billing?
The primary risks of outsourcing mental health billing are: hiring a generalist company without behavioral health expertise, losing visibility into your revenue cycle, and poor denial management. These risks are largely mitigated by choosing a billing partner that specializes in behavioral health, provides transparent real-time reporting, and has a documented denial management process. A HIPAA-compliant Business Associate Agreement (BAA) must be in place before sharing any patient data.
Can I outsource mental health billing and still stay HIPAA compliant?
Yes. Outsourcing billing is a standard, HIPAA-compliant practice when handled correctly. The billing company must sign a Business Associate Agreement (BAA) with your practice before accessing any protected health information (PHI). Any reputable billing company will have a standard BAA in place. Verify this before signing any contract.
How do I know if my current mental health billing is performing well?
Your billing is performing well if: your clean claim rate is 95%+ (meaning 95%+ of claims are accepted on first submission), your average days in accounts receivable (AR) is under 30, your denial rate is below 5%, and your collection rate is 95%+ of expected reimbursement. If you don’t know any of these numbers, the first step is a billing audit. Most practices that haven’t audited their billing discover they’re losing 10–20% of recoverable revenue.
What CPT codes are used for mental health billing?
The most common CPT codes for outpatient mental health billing include: 90791 (psychiatric diagnostic evaluation), 90837 (60-minute individual psychotherapy), 90834 (45-minute individual psychotherapy), 90832 (30-minute individual psychotherapy), 90847 (family psychotherapy with patient present), 90846 (family psychotherapy without patient present), and 90853 (group psychotherapy). These are time-based codes — accurate documentation of session start/stop times or total face-to-face time is required.
How does behavioral health insurance carve-out affect billing?
A behavioral health carve-out means the payer (e.g., Aetna, Cigna, Anthem) has contracted with a separate managed behavioral health organization (MBHO) — such as Optum Behavioral Health, Carelon Behavioral Health, or Magellan — to manage mental health benefits. This means you may need to credential separately with the MBHO, submit claims to a different entity, and follow different prior authorization and utilization management requirements than you would for the payer’s medical benefits.
What is the Mental Health Parity Act, and how does it affect billing?
The Mental Health Parity and Addiction Equity Act (MHPAEA) requires that insurance plans covering mental health and substance use disorder (SUD) benefits cannot apply more restrictive limitations than those applied to comparable medical/surgical benefits. In practical terms, this means that denial reasons, prior authorization requirements, and utilization management criteria for mental health services must be comparable to medical services. If a payer is denying mental health claims at higher rates or with stricter criteria than equivalent medical claims, it may constitute a parity violation — which can be appealed.
How long does mental health credentialing take?
Mental health credentialing with commercial insurance payers typically takes 60–120 days. Credentialing with behavioral health carve-out payers (Optum Behavioral Health, Carelon, Magellan) can take 90–150 days. Medicaid credentialing timelines vary dramatically by state — some state Medicaid programs take 6+ months. During this period, a clinician cannot bill in-network, which is why beginning the credentialing process as early as possible is critical for new practices and new hires.
Should a solo therapist in private practice outsource billing?
For most solo therapists, outsourcing billing makes practical and financial sense — particularly if they don’t have dedicated billing staff and are spending significant time on claims submission, denial follow-up, and credentialing. The key is finding a partner that specializes in mental health billing (not a generalist), charges a transparent percentage-of-collections fee, and provides clear reporting. Many solo therapists collect 10–15% more revenue after switching to a specialist billing partner because denial management improves significantly.
What should I look for when hiring a mental health billing company?
Look for: demonstrated specialization in behavioral health (not a generalist firm), transparency in reporting (live dashboard access), a clear denial management process, experience with behavioral health payer carve-outs, credentialing services, a dedicated account contact, and a HIPAA Business Associate Agreement (BAA). Ask for references from practices similar to yours. Avoid companies that can’t tell you their clean claim rate or that charge a flat fee per claim rather than a percentage of collections.
Is outsourcing billing a good option for a new mental health practice?
Yes — for most new mental health practices, outsourcing billing from day one is the most cost-effective and operationally sound approach. Building an in-house billing infrastructure requires hiring, training, software investment, and compliance oversight that is disproportionately burdensome for a practice that isn’t yet generating full revenue. Starting with an outsourced behavioral health billing specialist allows a new practice to focus on clinical care and growth while billing is handled by people who do it full-time.