Table of Contents
ABA billing is one of the most technically demanding billing environments in behavioral health, and one of the most expensive to get wrong
A clinic director at an autism therapy center described it well in a billing forum: “We spent six months trying to figure out why our Medicaid ABA claims kept getting denied. Turns out we were billing 97153 with the wrong rendering provider NPI; we needed the BT’s NPI, not the BCBA’s. Six months of resubmissions. Nobody told us this at enrollment.”
That’s ABA billing. It is technically specific, payer-variable, and unforgiving when documentation or modifier usage is off by one detail. The ABA CPT code set, introduced in 2019 when the AMA replaced older adaptive behavior codes, is more precise than most therapy billing codes. That precision is both the challenge and the solution. Get it right, and ABA claims pay cleanly. Get one detail wrong, and the same claim is denied every time.
This is the complete guide: every code, every modifier, every denial pattern, and every fix.
Free Download: Behavioral Health Billing & Coding Toolkit
Stop losing revenue with actionable frameworks that simplify — complex behavioral health billing rules.
Fill in your details to get instant access:
What Is ABA Billing and Why Is It More Complex Than Standard Therapy Billing?
ABA billing is the process of submitting claims for applied behavior analysis services, a clinical intervention for autism spectrum disorder and related conditions, using a specialized CPT code set that captures assessment, treatment, and supervision services at multiple provider levels.
What makes ABA billing uniquely complex:
- Tiered provider billing: ABA services are billed at different levels depending on who delivers the service, BCBA, BCaBA, RBT, or behavior technician. Each level may require a different modifier, a different rendering provider NPI, or a different claim format.
- Strict time-based unit rules: Most ABA CPT codes are billed in 15-minute units. Units must match the actual time documented in session notes, not the scheduled time or the estimated time.
- Supervision documentation requirements: BCBA supervision of RBT and BT sessions must be documented in a way that satisfies both clinical standards (BACB) and payer requirements, which are often different.
- Authorization complexity: ABA requires prior authorization from virtually every payer. Initial assessments, treatment plans, and ongoing services each have separate authorization requirements with strict renewal windows.
- State-level Medicaid variation: Medicaid ABA coverage, covered codes, supervision ratios, and authorization processes vary significantly by state; what works in Texas fails in California.
What Are the Core ABA CPT Codes and When Do You Use Each One?
The ABA CPT code set (97151–97158) was introduced in January 2019, replacing the adaptive behavior codes (0359T–0374T). Here is the complete reference:
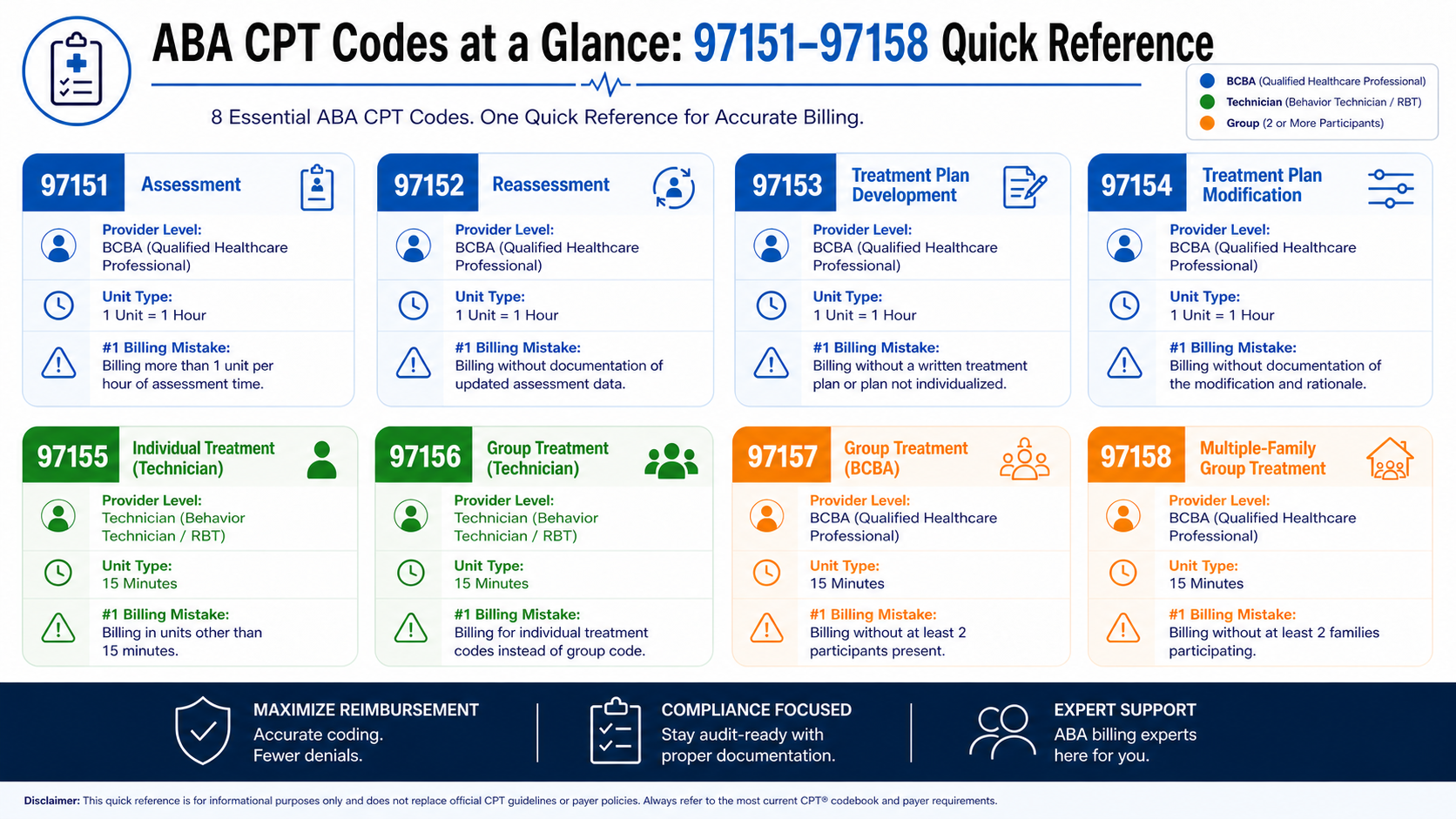
Full ABA CPT Code Reference Table
| CPT Code | Service Description | Provider Level | Unit Type |
|---|---|---|---|
| 97151 | Behavior identification assessment | BCBA/BCaBA | Per 15 minutes |
| 97152 | Behavior identification supporting assessment | Technician (supervised) | Per 15 minutes |
| 97153 | Adaptive behavior treatment by protocol | Technician (supervised) | Per 15 minutes |
| 97154 | Group adaptive behavior treatment by protocol | Technician (supervised) | Per 15 minutes |
| 97155 | Adaptive behavior treatment with protocol modification | BCBA/BCaBA | Per 15 minutes |
| 97156 | Family adaptive behavior treatment guidance | BCBA/BCaBA | Per 15 minutes |
| 97157 | Multiple-family group adaptive behavior treatment guidance | BCBA/BCaBA | Per 15 minutes |
| 97158 | Group adaptive behavior treatment with protocol modification | BCBA/BCaBA | Per 15 minutes |
What Is CPT Code 97151 and When Is It Used?
97151 is the behavior identification assessment, the initial clinical assessment conducted by a BCBA or BCaBA to determine diagnosis, behavioral function, and treatment plan. This maps to the VB-MAPP, ABLLS-R, or similar standardized assessment.
- Billed in 15-minute units by the BCBA
- Most payers require prior authorization before the 97151 assessment begins
- Documentation: assessment instrument used, raw scores, behavioral observations, function hypothesis, and treatment recommendations
Common mistake: Billing 97151 without confirming assessment authorization is separate from treatment authorization; they are billed and authorized separately at most payers
What Is CPT Code 97152 and How Is It Different From 97151?
97152 is the behavior identification supporting assessment, the data collection and probing activities conducted by a behavior technician under BCBA supervision, in support of the assessment.
- Billed by the supervising BCBA’s NPI (or the BT’s NPI with appropriate modifier, depending on payer)
- Must be concurrent with or directly supporting the 97151 assessment
Common mistake: Billing 97152 as a standalone service without 97151 billed on the same or adjacent dates, payers require 97152 to be associated with an active assessment
What Is CPT Code 97153 and What Documentation Does It Require?
97153 is adaptive behavior treatment by protocol, direct one-on-one ABA therapy delivered by a behavior technician (RBT) under BCBA supervision. This is the highest-volume code in ABA billing.
- Billed in 15-minute units
- The rendering provider on the claim is typically the BT/RBT’s NPI (payer-specific)
- BCBA supervision must be documented: supervision ratio, type of supervision (direct vs. indirect), and BCBA co-signature on session notes where required
Most common denial reason: Rendering NPI does not match the enrolled technician, which happens frequently when multiple BTs cover cases
What Is CPT Code 97154 and When Does It Apply?
97154 is group adaptive behavior treatment by protocol, 97153 delivered in a group setting (2 or more clients simultaneously).
- Billed per client, per session, not one unit for the whole group
- Group size limits vary by payer (typically 2–8 clients; confirm per payer)
- BCBA supervision documentation must cover the group session
Common mistake: Billing 97154 without confirming the payer covers group ABA; some Medicaid plans do not reimburse group format without specific authorization
What Is CPT Code 97155 and What Are Its Billing Rules?
97155 is adaptive behavior treatment with protocol modification, the time the BCBA spends directly with the client and BT, modifying the behavior intervention plan in real time. This is the BCBA’s direct service code.
- Billed in 15-minute units by the BCBA
- Can be billed on the same date as 97153 (BCBA is present, supervising while BT implements protocol)
- Time overlap rule: 97155 and 97153 can be billed simultaneously, the BCBA’s protocol modification time and the BT’s treatment time run concurrently. Document the total time for each separately.
Common mistake: Not billing 97155 when the BCBA is present and providing direct protocol modification. This is one of the most consistently underbilled codes in ABA.
What Is CPT Code 97156 and How Is Family Training Billed?
97156 is family adaptive behavior treatment guidance, direct training provided by a BCBA to family members or caregivers, without the client present.
- Billed in 15-minute units by the BCBA
- Caregiver must be present; client does not need to be
- Requires separate documentation from the client’s session note; the parent/caregiver training note must document objectives, content, caregiver response, and plan
Common mistake: Not billing 97156 for caregiver training sessions that are already occurring but never billed. This is a frequently missed revenue source.
Are You Billing 97155 and 97156 Every Time You Should Be?
Most ABA clinics underbill for BCBA protocol modification (97155) and caregiver training (97156) because no one tracks them systematically. At a 10-client clinic, that’s $3,000–$8,000 in missed monthly revenue.
What Is CPT Code 97157 and When Is It Used?
97157 is a multiple-family group adaptive behavior treatment guidance, the same service as 97156, but delivered to 2+ families simultaneously.
- Billed per family unit, per session
- Less commonly billed; payer coverage varies, always confirm authorization covers the group format.
What Is CPT Code 97158 and What Are Its Unit Rules?
97158 is group adaptive behavior treatment with protocol modification, BCBA-level group treatment involving active protocol modification.
- Billed per client in the group
- Used when the BCBA is directly providing protocol modification in a group format
- Rarely billed; most group ABA services use 97154. Use 97158 only when BCBA-level protocol modification (not just supervision) is occurring.
What Modifiers Are Required for ABA Insurance Billing?
ABA billing modifiers communicate the provider level, setting, and clinical context to payers. Wrong or missing modifiers are the second most common cause of ABA denials after authorization issues.
Core ABA Modifier Reference Table
| Modifier | Meaning | Used With |
|---|---|---|
| HN | Bachelor's level provider | 97153, 97154 (BT/RBT with bachelor's degree) |
| HO | Master's level provider | 97153, 97155 (BCaBA or master's-level BCBA) |
| HP | Doctoral-level provider | 97151, 97155 (doctoral-level BCBA) |
| HQ | Group setting | 97154, 97157, 97158 |
| GT | Telehealth, synchronous audio/video | Telehealth ABA services |
| 95 | Synchronous telemedicine | Alternative to GT (payer-specific) |
| TT | Competitive employment incentive | State Medicaid programs (select states) |
| U1–U9 | State-specific modifiers | Varies by state Medicaid program |
What Is the Difference Between HN, HO, and HP Modifiers in ABA Billing?
These modifiers communicate the education and credential level of the rendering provider, not their role:
- HN (bachelor’s level): Used when the rendering technician holds a bachelor’s degree, typically an RBT or BT with a bachelor’s in psychology, education, or a related field
- HO (master’s level): Used when the rendering provider holds a master’s degree, BCaBA, or BCBA at the master’s level
- HP (doctoral level): Used when the rendering BCBA holds a doctoral degree
The billing reality: Not all payers require HN/HO/HP modifiers for ABA claims; some Medicaid programs require them; many commercial payers don’t. Submit without them to commercial plans that don’t require them; add them to Medicaid plans that do. Billing HN/HO/HP to a payer that doesn’t accept these modifiers can trigger a CO-16 or CO-4 denial.
When Are State-Specific Modifiers Required for ABA Medicaid Billing?
Many state Medicaid programs require U-series modifiers (U1–U9) to communicate ABA-specific information, supervision type, service setting, or provider authorization level. These are entirely state-specific:
- Texas Medicaid: Requires specific modifiers for BCBA supervision type (direct vs. indirect)
- Florida Medicaid: Modifier requirements vary by managing entity
- California Medi-Cal: Magellan-managed ABA has its own modifier guidance
Confirm state-specific modifier requirements with each Medicaid managed care organization before the first submission.
How Does ABA Time-Based Billing Work, and Where Do Providers Get It Wrong?
ABA CPT codes are billed in 15-minute units. The number of units billed must match the actual face-to-face or direct service time documented in the session note, not the scheduled time or authorization limit.
The correct unit calculation:
- 60 minutes of 97153 = 4 units
- 90 minutes of 97153 = 6 units
- 45 minutes of 97155 concurrent with 60 minutes of 97153 = 3 units of 97155 + 4 units of 97153
The most common time billing errors:
- Billing scheduled time instead of actual time: A 90-minute scheduled session that runs 78 minutes should be billed as 5 units (75 minutes), not 6. Billing scheduled time when actual time differs is overcoding.
- Not accounting for concurrent billing: When 97155 and 97153 run simultaneously, both codes are billed for their respective time. The total billable units may exceed the total session length; this is correct, not a billing error.
Rounding up to the next unit threshold: ABA uses an “8-minute rule” for the final partial unit (per AMA guidance). A unit of 15 minutes requires 8+ minutes of service. Not all payers follow AMA rounding rules; confirm per payer.
Why Do ABA Claims Get Denied, and What Are the Most Common Causes?
Top ABA Denial Reasons
| Denial Reason | Denial Code | Fixes |
|---|---|---|
| No prior authorization | CO-15 | Never submit without confirmed auth; verify before every date of service |
| Auth expired | CO-97 | Track auth end dates; initiate renewal 3 weeks before expiration |
| Wrong rendering NPI | CO-16 | Confirm BT/RBT is enrolled and the NPI matches the claim exactly |
| Documentation mismatch | CO-11 | Session note units must match billed units to the minute |
| Wrong modifier | CO-4 | Confirm modifier requirements per payer before the first claim |
| Supervision ratio not met | CO-11 | BCBA supervision ratio documentation must be in the session note |
| BCBA not credentialed | CO-4 | BCBA must be enrolled with both the commercial payer AND MBHO if carved out |
| Concurrent billing is not allowed | CO-97 | Some payers don't allow 97153 + 97155 on the same claim; confirm per payer |
How Do Authorization Gaps Cause ABA Billing Denials?
ABA has one of the most intensive prior authorization environments in all of behavioral health. Every stage requires separate authorization:
- Assessment authorization (97151, 97152), separate from treatment
- Treatment authorization, typically 6 months, requires renewal with an updated treatment plan
- Concurrent review, some payers require mid-authorization clinical reviews
An ABA clinic with 30 active patients and 6-month auth cycles has approximately 5 authorizations expiring every month. Without systematic tracking, lapses are inevitable, and every date of service after an auth lapses is a retroactive denial.
What Documentation Mismatches Trigger ABA Claim Denials?
Payers increasingly conduct post-payment documentation reviews for ABA claims. The most common mismatches:
- Session notes document 4 units (60 minutes) of 97153; claim billed 6 units
- BCBA supervision was noted in the record as “indirect,” but the modifier indicates direct supervision
- Caregiver training (97156) billed, but no caregiver present per session note
- Group session (97154) billed for 8 clients, but documentation only lists 5 present
How Does ABA Billing Differ Between Medicaid and Commercial Payers?
| Factor | Medicaid | Commercial (MBHO) |
|---|---|---|
| CPT codes accepted | 97151–97158 (state-specific variations) | 97151–97158 (with MBHO-specific rules) |
| Modifier requirements | Often required (HN/HO/HP + state modifiers) | Varies; some plans don't require |
| Authorization | Required; state MCO-specific | Required; MBHO-specific |
| BCBA supervision ratio | State-specific documentation requirement | Payer-specific |
| Concurrent billing (97153+97155) | Some states disallow | Most commercial plans allow |
| Telehealth coverage | State-specific; many allow post-COVID | Most allow with modifier 95/GT |
| Rendering NPI rules | Often requires BT/RBT NPI | Varies; some accept BCBA NPI for all |
The most important Medicaid vs. commercial distinction: Many state Medicaid programs require the BT/RBT’s individual NPI on 97153 claims, not the BCBA’s. Most commercial payers accept the BCBA’s NPI as the rendering provider for all ABA codes. Submitting the wrong NPI to either payer type is a denial that can be avoided entirely with a payer-specific billing reference.
ABA Billing Is Too Complex for a Generalist Billing Team.
The difference between an ABA billing specialist and a general biller is measured in denial rates, auth lapses, and missed 97155/97156 charges, month after month. BehavioralProz handles ABA billing exclusively within behavioral health, with the CPT expertise, modifier knowledge, and payer relationships your clinic needs.
What Are the Most Common ABA Billing Mistakes That Cost Clinics Revenue?
- Not billing 97156 for caregiver training, routinely occurring, routinely not billed. At $60–$100/unit, this is consistent monthly revenue left unclaimed.
- Not billing 97155 when BCBA is present, the BCBA’s protocol modification time during 97153 sessions is separately billable but frequently not captured. At a 10-client clinic with daily BCBA supervision, this is $3,000–$8,000/month in recoverable revenue.
- Billing scheduled units instead of actual units, systematic overcoding that creates audit risk without generating additional revenue.
- Using the same NPI for all ABA codes regardless of payer works for some commercial plans, but fails for most Medicaid plans.
- Auth renewal not initiated before expiration is the most expensive single mistake, because every session after auth lapses is denied retroactively.
- Credentialing BCBA with commercial plan but not with MBHO, BCBA credentialed with Aetna but not Evernorth/Cigna Behavioral Health; ABA claims denied for non-credentialed provider.
What Does a Clean ABA Billing Workflow Look Like?
Daily:
- Session notes completed and signed before billing runs
- Units documented match billed units exactly
- Rendering NPI confirmed for each BT/RBT before claim submission
Weekly:
- Authorization status confirmed for every active patient
- Any authorization expiring within 21 days is flagged for renewal
- Denied claims worked within 10 business days
Monthly:
- Denial trend analysis by denial code and payer
- 97155 and 97156 audited. Are all BCBA supervision and caregiver training sessions being captured?
- AR aging review, any ABA claim over 60 days flagged for escalation
Quarterly:
- Coding audit, 10 sessions per clinician, compared against billed units
- Credentialing status review, every BCBA and BT is active with every payer
ABA Billing Gets Easier When Every Detail Has a System
ABA billing doesn’t fail because providers don’t care. It fails because the details are numerous, payer-specific, and unforgiving: a wrong NPI on a 97153 claim, a missed modifier, an auth that expired on a Friday, and a 97155 that ran but was never captured.
The CPT codes are precise by design. That precision works in your favor when documentation, modifiers, rendering providers, and authorization windows are all managed systematically. It works against you when any one of those variables slips.
The clinics that bill ABA cleanly aren’t doing anything complicated. They’re running the same daily, weekly, and monthly checks every time, for every patient, across every payer. The workflow in this guide is where that starts.
If your denial rate is climbing or your 97155 and 97156 charges aren’t showing up in your revenue, those are solvable problems, and they almost always trace back to a specific gap in the billing process, not a systemic failure. If you’re weighing whether to outsource, it’s worth running the numbers on how contingency and flat-fee billing costs compare before choosing a vendor structure.
ABA Billing Is Just One Part of Running a Profitable Autism Therapy Clinic.
The Behavioral Health Operations Playbook covers ABA billing workflows, denial prevention, authorization management, RCM KPIs, and operational benchmarks, everything an ABA clinic needs to run efficiently and profitably.
Frequently Asked Questions
What are the most common ABA CPT codes?
CPT codes 97153 (direct therapy by technician), 97155 (BCBA protocol modification), and 97151 (behavior assessment) are the most frequently billed ABA codes.
What is CPT code 97153 used for in ABA billing?
97153 is used for one-on-one adaptive behavior treatment delivered by a behavior technician under BCBA supervision, the most common ABA direct service code, billed in 15-minute units.
Can 97153 and 97155 be billed on the same day?
Yes, 97153 (BT direct treatment) and 97155 (BCBA protocol modification) can be billed concurrently when the BCBA is present and actively modifying the protocol during the BT’s session.
Why do ABA claims get denied?
Missing or expired prior authorization, incorrect rendering provider NPI, wrong or missing modifiers, and documentation mismatches (billed units don’t match the session note) are the leading causes of ABA denials.
What modifiers are used in ABA billing?
The most common ABA modifiers are HN (bachelor’s level), HO (master’s level), HP (doctoral level), and HQ (group setting). State Medicaid programs may also require U-series modifiers; confirm per state.
How are ABA billing units calculated?
ABA CPT codes are billed in 15-minute units based on actual face-to-face time documented in the session note, not scheduled time. A 60-minute session = 4 units. A partial unit of 8+ minutes rounds up to one unit per AMA guidance (verify per payer).
Does Medicaid cover ABA therapy?
Yes, most state Medicaid programs cover ABA therapy for children with ASD, managed through MCOs or RBHAs. Coverage age limits, authorized codes, supervision requirements, and authorization processes vary by state.
What is the difference between CPT 97151 and 97155 in ABA?
97151 is the initial behavior identification assessment (evaluation); 97155 is ongoing adaptive behavior treatment with protocol modification by a BCBA during active treatment. They serve different purposes at different stages of care.
How often does ABA authorization need to be renewed?
Most payers require ABA authorization renewal every 6 months, with an updated treatment plan and concurrent review documentation. Some payers require interim reviews at 3 months. Track expiration dates proactively; authorization lapses are the top cause of retroactive ABA denials.