Table of Contents
A behavioral health practice director managing clinics in three states put it plainly: “I learned very quickly that what works in Georgia does not work in North Carolina. Same provider. Same service. Different Medicaid managed care organization, different authorization system, different billing code set. We lost thousands in denials before we figured it out.”
That’s the reality of behavioral health billing in the U.S. There is no single national standard. Medicaid, which covers approximately 40% of behavioral health utilization nationally, is administered separately in every state. Commercial payer rules layer on top of that. Add telehealth policy variation, ABA authorization differences, and MBHO carve-out complexity, and you have a billing environment where geography is as important as clinical expertise.
This guide covers the billing landscape in every major state, what’s different, what causes denials, and what providers operating across state lines need to know.
Why Does Behavioral Health Billing Vary So Much by State?
Behavioral health billing varies by state primarily because Medicaid is a federal-state partnership; each state designs its own program within federal guidelines. This means each state controls:
- Which behavioral health services are covered?
- Which provider types are eligible to bill?
- How prior authorization is managed (and by whom)?
- Whether behavioral health is carved out to a separate managed care organization?
- What telehealth modalities and codes are accepted?
- What documentation standards apply?
Commercial payers add additional variation, particularly because MBHO carve-outs (Optum, Carelon, Magellan) operate under state-specific contracts with different rules in each state.
The result: a BCBA billing ABA in Texas faces different rules than a BCBA billing ABA in California or New York. An LCSW credentialing with Medicaid in Florida navigates a different system than an LCSW in Pennsylvania. Multi-state practices that treat these differences as minor administrative variations consistently lose revenue they didn’t know was at risk.
What Provider Types Are Affected Most by State Billing Differences?
| Provider Type | Highest State Variation Risk |
|---|---|
| BCBAs / ABA Therapists | Medicaid ABA covered codes, auth requirements, RBT billing rules |
| LCSWs / LPCs / LMFTs | Medicaid eligible provider lists, independent billing scope by state |
| Psychiatric NPs (PMHNPs) | Prescriptive authority, collaborative agreement requirements, and Medicaid enrollment |
| SUD Counselors (CADCs) | Credential level requirements for Medicaid billing eligibility |
| Psychologists | Medicare/Medicaid enrollment, neuropsychological testing coverage |
| Group Practices | Medicaid MCO contracting, group NPI enrollment requirements by state |
How Do You Bill Behavioral Health Services in California?
California Medicaid (Medi-Cal) is one of the most complex behavioral health billing environments in the U.S., and one of the highest-stakes, given the state’s population.
What Are the Biggest Medi-Cal Billing Challenges for Behavioral Health Providers?
- Specialty Mental Health Services (SMHS) vs. Non-Specialty MHS: California divides behavioral health into “specialty” (county-administered) and “non-specialty” (Managed Care Plan-administered), a split that confuses out-of-state providers and creates dual enrollment requirements.
- ABA billing: Medi-Cal covers ABA for members under 21 with ASD; authorization managed through Magellan, requires BCBA supervision documentation for every BT/RBT session billed under H2019.
- Telehealth: California allows synchronous audio-only telehealth for behavioral health (a permanent post-COVID policy), but modifier and POS requirements apply; Document audio-only sessions with specific consent language.
- Provider enrollment: California county mental health plans require separate enrollment from Medi-Cal Managed Care Plans; solo providers and group practices must often enroll in multiple systems.
- Common denial: “Service not authorized”, particularly for SMHS claims routed to county systems when the member was enrolled in Medi-Cal Managed Care.
Billing Behavioral Health Services in Multiple States? You Need a Specialist, Not a Generalist.
State Medicaid rules, MCO enrollment, ABA authorization, SUD licensing requirements, multi-state behavioral health billing fails in predictable places. BehavioralProz manages billing across all 50 states with state-specific expertise.
How Do You Bill Behavioral Health Services in Texas?
Texas Medicaid behavioral health (managed by STAR Health, STAR+PLUS, and Texas CHIP) is administered through multiple managed care organizations, each with its own prior auth rules and billing requirements.
Why Is Texas Medicaid ABA Authorization So Complex?
Texas Medicaid ABA coverage for autism spectrum disorder is managed through the STAR Health MCOs and requires:
- Diagnosis of ASD via an approved diagnostic instrument.
- Initial authorization for assessment (H0031/H0032) before treatment authorization.
- 6-month treatment authorization renewals with concurrent review documentation.
- BCBA supervision ratios documented per session.
Common Texas-specific billing issues:
- Billing direct therapy hours (H2019) without documented BCBA supervision ratio triggers denial.
- Texas Medicaid requires the rendering NPI on ABA claims to match the enrolled BT or BCBA, not a generic group NPI.
- Telehealth: Texas expanded telehealth permanently post-COVID, but audio-only behavioral health has specific coverage criteria per MCO; confirm per plan.
How Do You Bill Behavioral Health Services in Florida?
Florida Medicaid behavioral health is managed through seven Regional Behavioral Health Managing Entities (ME), each operating independently with its own provider network and billing processes.
Key Florida billing considerations:
- Provider enrollment: Behavioral health providers must enroll with Florida Medicaid AND with the managing entity in their region. Billing Florida Medicaid without ME enrollment triggers denials.
- ABA billing: Florida Medicaid covers ABA for children with ASD, managed through MEs with prior auth; documentation must reflect BCBA supervision notes.
- Baker Act: Providers treating involuntary patients under the Baker Act must understand distinct billing codes and Medicaid managed care coordination rules.
- SUD billing: Florida uses DCF-licensed providers for SUD treatment. Medicaid SUD billing requires DCF certification.
- Telehealth: Florida allows telehealth behavioral health, but specific platforms and consents apply; audio-only has variable MCO coverage.
- Common denial: Wrong managing entity billing address or submitting to Medicaid directly when the ME manages the benefit.
How Do You Bill Behavioral Health Services in New York?
New York has one of the most layered behavioral health billing environments in the country, with distinct rules across Medicaid, HARP (Health and Recovery Plan), commercial plans, and OPWDD.
Key New York billing considerations:
- HARP enrollment: Adults with serious mental illness or SUD enrolled in HARP access Home and Community Based Services (HCBS), a distinct billing pathway separate from standard OMH billing.
- Article 31 / Article 16 licensing: Outpatient mental health clinics (Article 31) and OPWDD facilities (Article 16) have facility-specific billing requirements, rates, and documentation standards.
- OMH licensed providers vs. independent practitioners: Licensed OMH clinics bill differently than solo practitioners; rates, codes, and enrollment pathways differ
- ABA billing: Medicaid ABA in New York is managed through MCOs; OPWDD manages services for individuals with developmental disabilities separately.
- Telehealth: New York permanently expanded telehealth post-COVID; audio-only covered for behavioral health with proper consent documentation.
- Common denial: Billing Article 31 services under an individual NPI when a facility NPI is required.
How Do You Bill Behavioral Health Services in Illinois?
Illinois Medicaid behavioral health is managed through Managed Care Organizations (MCOs), including IlliniCare, Meridian, and Molina, each operating under the HealthChoice Illinois program.
Key Illinois billing considerations:
- MCO-specific enrollment is required for each plan: Illinois Medicaid fee-for-service is increasingly limited.
- ABA billing: Illinois Medicaid covers ABA for ASD, prior auth required; MCOs manage authorization independently with varying documentation standards.
- DHS-licensed SUD providers must maintain DHS certification for Medicaid SUD billing eligibility.
- Telehealth: Illinois made telehealth parity permanent, audio/video both reimbursable for behavioral health at the same rates as in-person.
- Common denial: Billing Illinois Medicaid fee-for-service for patients enrolled in an MCO; confirm MCO enrollment before every claim.
How Do You Bill Behavioral Health Services in Pennsylvania?
Pennsylvania Medicaid behavioral health (HealthChoices) is managed through county-based Behavioral Health Managed Care Organizations (BH-MCOs), one per county.
Key Pennsylvania billing considerations:
- County BH-MCOs contract independently; A provider enrolled with Community Care Behavioral Health (CCBH) in Allegheny County is not automatically enrolled in CBH in Philadelphia.
- SUD billing: DDAP-licensed facilities bill through county BH-MCOs under specific HCPCS codes with utilization management requirements.
- ABA billing: PA Medicaid covers ABA through the Physical Health MCOs (not BH-MCOs), a separate enrollment from behavioral health Medicaid.
- Telehealth: PA maintains expanded telehealth post-COVID, with audio-only covered for behavioral health.
- Common denial: Billing the wrong county, BH-MCO, for a member who recently moved counties. Verify the county of enrollment before claims are submitted.
How Do You Bill Behavioral Health Services in Ohio?
Ohio Medicaid behavioral health is managed through Managed Care Plans, including Anthem, Buckeye, CareSource, Molina, and UnitedHealthcare Community Plan.
Key Ohio billing considerations:
- Behavioral health carve-in: Ohio carved behavioral health back into Medicaid MCOs from a carve-out model; providers must re-enroll with each MCO separately
- SUD billing: OhioMHAS certification required for SUD Medicaid billing; HCPCS H-codes required for most SUD services.
- ABA billing: Ohio Medicaid covers ABA, prior auth managed by MCOs; Ohio has specific BCBA supervision ratio documentation requirements.
- Telehealth: Ohio allows audio and video telehealth for behavioral health; MCO-specific coverage details vary.
- Common denial: Incorrect place of service code on telehealth claims, Ohio MCOs are strict on POS 10 vs. POS 02.
Did Your State's Medicaid Rules Change This Year? Ours Tracks Every Update.
Medicaid behavioral health programs change annually, new MCO contracts, new authorization requirements, and new code sets. Providers that don’t track changes see their denial rate climb. BehavioralProz keeps your billing current with every state’s current rules.
How Do You Bill Behavioral Health Services in Georgia?
Georgia Medicaid behavioral health is managed through three Care Management Organizations (CMOs): Amerigroup, CareSource, and WellCare (now Centene).
Key Georgia billing considerations:
- CMO-specific enrollment required: Providers must be credentialed separately with each CMO.
- DBHDD licensing: Behavioral health facilities and SUD programs must maintain DBHDD licensure for Medicaid billing eligibility.
- ABA billing: Georgia Medicaid covers ABA; CMOs manage authorization; RBT supervision documentation required.
- Georgia implemented a significant Medicaid managed care expansion, and providers who were enrolled in fee-for-service must re-enroll with CMOs.
- Telehealth: Georgia allows telehealth for behavioral health, and post-COVID expansions have been made permanent for most service types.
- Common denial: DBHDD license expired or was not updated in the CMO credentialing files.
How Do You Bill Behavioral Health Services in North Carolina?
North Carolina Medicaid behavioral health is managed through Local Management Entities-Managed Care Organizations (LME-MCOs), seven regional entities covering distinct geographic areas.
Key North Carolina billing considerations:
- LME-MCO enrollment is mandatory and regional: A provider cannot bill NC Medicaid BH without enrollment in the LME-MCO covering their service area.
- NC Medicaid Tailored Plans (behavioral health specialty MCOs) launched in 2023: Providers serving members with serious mental illness or SUD must now enroll with Tailored Plans separately from standard Medicaid MCOs.
- ABA billing: Managed through Tailored Plans; North Carolina has specific BCBA supervision and documentation requirements.
- SUD billing: NC Medicaid SUD billing requires DMH/DD/SAS certification; HCPCS H-codes required.
- Telehealth: NC allows audio and video telehealth with post-COVID permanency for behavioral health.
- Common denial: Billing standard MCO for a member enrolled in a Tailored Plan after the 2023 transition.
How Do You Bill Behavioral Health Services in Arizona?
Arizona Medicaid (AHCCCS) behavioral health has a unique structure, the most integrated in the country, with Regional Behavioral Health Authorities (RBHAs) managing all behavioral health services.
Key Arizona billing considerations:
- RBHA enrollment: All behavioral health providers must be credentialed with the RBHA covering their region, Mercy Maricopa (Maricopa County), Southwest Network, Cenpatico Behavioral Health, or the tribal RBHA
- ABA billing: AHCCCS covers ABA for members with ASD, managed through RBHAs with prior auth and BCBA supervision requirements
- SUD billing: AHCCCS covers SUD treatment; DBHS certification required; H-codes required
- Integrated model: Arizona has one of the most integrated BH/physical health systems, providers billing both must navigate dual enrollment in RBHA and AHCCCS Complete Care plans
- Telehealth: Arizona allows audio and video telehealth; RBHA-specific coverage details apply
- Common denial: Missing or incorrect RBHA routing, claims submitted without RBHA enrollment are actively denied across the board
What About Other Key U.S. States?
| State | Key Billing Consideration |
|---|---|
| New Jersey | FamilyCare MCOs manage BH; separate DHS credentialing is required for SUD providers |
| Michigan | PIHPs (Prepaid Inpatient Health Plans) manage BH, CMH enrollment separately from Medicaid |
| Virginia | DMAS MCOs manage BH; DBHDS licensure required; BH carved into MCOs since 2022 |
| Colorado | Regional Accountable Entity (RAE) model, BH integrated; RAE enrollment required |
| Washington | Apple Health MCOs manage BH; BHA certification required for SUD billing |
| Massachusetts | MassHealth MCOs; CBHI manages youth BH; SUD billing through BSAS-licensed providers |
| Tennessee | TennCare MCOs (BlueCare, UNUM); separate enrollment per plan required |
| Indiana | Managed care MCOs handle BH; PathWays program launching for LTSS/BH integration |
| Missouri | MO HealthNet MCOs; SUD billing requires a DMHA-licensed facility |
| Nevada | Nevada Medicaid BH managed by Anthem and SilverSummit; ABA is rapidly expanding |
What Should Multi-State Behavioral Health Organizations Know About Billing Across States?
Multi-state operations are where billing complexity compounds fastest. The same clinical service may require:
- A different HCPCS or CPT code in each state
- A different MCO or RBHA for claims routing
- A different prior authorization process and timeline
- A different documentation standard for medical necessity
- Separate credentialing with each state’s managed care organizations
The critical operational requirements for multi-state billing:
- State-specific payer matrix: Document the correct MCO, code set, modifier, and auth process for each state you operate in. Update it when Medicaid programs change (which happens annually in most states)
- Separate credentialing tracking by state. Each state’s Medicaid enrollment is independent. A provider credentialed in Georgia is not enrolled in North Carolina. Track each state separately.
- Telehealth billing by state, Telehealth policies have stabilized post-2020 but vary on audio-only coverage, consent requirements, and platform specifications. Maintain a state-specific telehealth billing reference.
SUD billing compliance by state. State licensing requirements for SUD facilities (DBHDD, DMHA, DDAP) affect billing eligibility at the state level. Lapsed state certifications trigger Medicaid billing suspension.
What Are the Most Common State-Specific Billing Mistakes That Cost Providers Revenue?
| Mistake | States Most Affected | Revenue Impact |
|---|---|---|
| Billing Medicaid fee-for-service for MCO-enrolled member | All MCO states | Full claim denial |
| Wrong MCO/RBHA routing | GA, AZ, NC, PA, IL | Full claim denial |
| Missing the state facility license on the claim | CA, TX, FL, PA, NC | Claim hold or denial |
| The BCBA supervision ratio is not documented | TX, CA, FL, NY, OH | ABA claim denial |
| Audio-only telehealth without consent documentation | CA, NY, WA | Medical record request or denial |
| Expired CAQH profile at state MCO re-attestation | All states | Provider enrollment suspension |
| SUD H-codes billed without state certification | All SUD states | Full claim denial |
Multi-State Billing Is Complex. Your Operations Playbook Shouldn't Be.
The Behavioral Health Operations Playbook covers billing workflows, denial prevention, multi-state RCM strategy, and KPI benchmarks, everything a behavioral health organization needs to operate efficiently across states.
Frequently Asked Questions
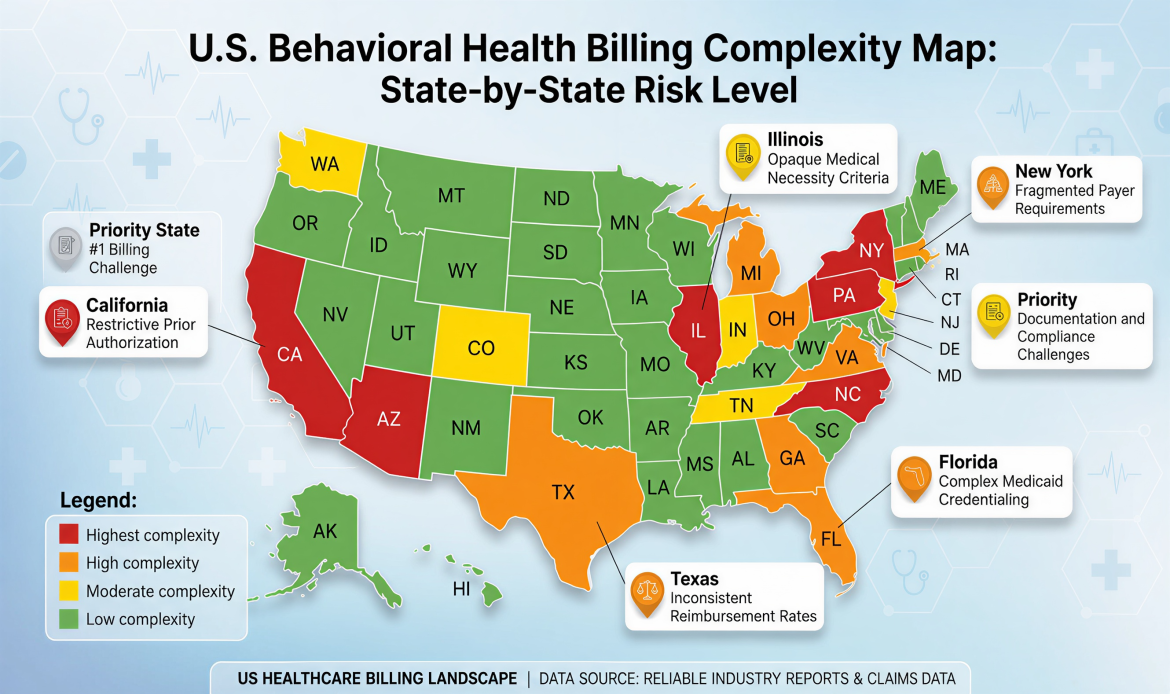
Which state has the most complex behavioral health Medicaid billing rules?
California, New York, and North Carolina are consistently the most complex, due to split Medicaid systems, RBHA/LME-MCO structures, and specialty licensing requirements.
Does ABA billing differ by state?
Yes, significantly. Medicaid ABA coverage, authorization requirements, BCBA supervision ratio documentation, and covered CPT/HCPCS codes vary by state and MCO.
What is an RBHA, and how does it affect behavioral health billing in Arizona?
A Regional Behavioral Health Authority (RBHA) manages all Medicaid behavioral health services in Arizona. Providers must be credentialed with the RBHA in their region before billing any AHCCCS behavioral health claims.
Do behavioral health providers need to credential separately in each state for Medicaid?
Yes. Each state’s Medicaid program and managed care organizations require separate enrollment. Credentialing with commercial payers is also state-specific.
What is the difference between a Medicaid MCO and a Medicaid carve-out in behavioral health billing?
An MCO integrates behavioral health into the managed care plan. A carve-out routes behavioral health to a separate MBHO (Optum, Carelon, Magellan), requiring different enrollment, authorization, and claims submission processes.
Can behavioral health providers bill telehealth in all states?
Yes, all 50 states allow some form of telehealth for behavioral health post-COVID, but audio-only coverage, platform requirements, modifier usage, and documentation requirements vary by state and payer.
Why do behavioral health Medicaid claims get denied in multi-state practices?
The most common reasons are wrong MCO routing, billing state fee-for-service for MCO-enrolled members, missing state facility licensing, and expired provider enrollment in one state’s Medicaid program.
What is the LME-MCO system in North Carolina behavioral health billing?
Local Management Entities-Managed Care Organizations (LME-MCOs) are regional entities that manage Medicaid behavioral health benefits in North Carolina. Providers must be credentialed with the LME-MCO covering their geographic service area.